Have you ever tried troubleshooting a problem so much that you start to feel insane, and then like magic, the solution to it becomes clear and you wonder why you hadn’t tried it earlier?
This was the case with me and the mysterious high blood sugars that plagued me for two and a half days.
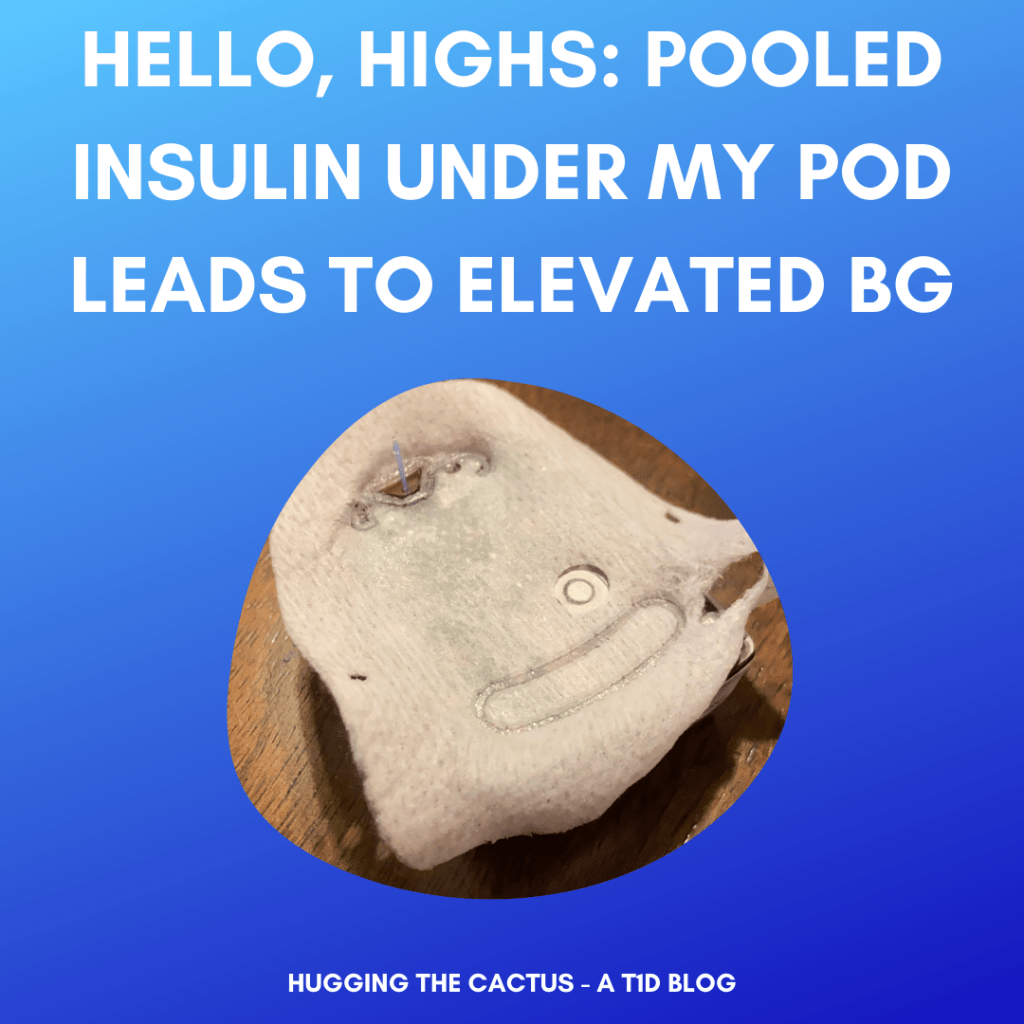
Based on this image, can you tell what was causing my blood sugar to be stubbornly high?
Once I started noticing a pattern of high blood sugars that got worse every time I ate food, I started doing everything else except changing my pod. I tried taking insulin for double the amount of carbs that I was actually eating, I ran a 95% temp basal increase for 8 out of 24 hours in the day, I cut carbs altogether and ate only 0 carb foods, I skipped meals altogether, and I even tried marching around the house for 15-minute intervals to try to get my insulin pumping through my system faster.
And nothing worked. I was able to get my blood sugar no lower than 180, but for most of that 60-hour window of time, I spent a good chunk of it in the mid-to-upper 200s.
Finally, on the day that my pod was due for a change, I decided that it must be the culprit behind my high blood sugars. When I removed the old pod, I knew immediately that something was wrong because the smell of insulin was so strong; plus, there was a large, damp spot on the pod’s adhesive, indicating that perhaps my insulin was pooling under my pod instead of entering my body.
It took 5-6 hours after I removed the leaky pod, but I finally did start to come back down to my normal levels, and was totally back on track the next day. It was a frustrating experience to endure, but a stark reminder of something that I’ve known in the back of my mind for years: that when I’m in doubt, I should change my pod.
Have you ever noticed that certain activities have a swift and obvious impact on your blood sugar levels?
Well, if you aren’t a person with diabetes, then the answer to that is probably “no”…but I digress! Recently, I realized that there are five things that absolutely, definitely, without-a-doubt make my blood sugar plummet before long. Here’s my list – what’s on yours?
1 – Vacuuming. I live in a fairly small condo – less than 900 square feet total – but when it comes time to vacuuming the floor, it takes me a good chunk of time to do a thorough job. Maybe about 30 minutes total. So it shouldn’t be surprising that by the time I’m done, I’m normally a little sweaty and often in need of a snack because all that moving around has made my blood sugar drop.
Who else “celebrates” vacuuming their entire home by cracking open a fresh…juice box??
2 – Baking. This might be surprising because I’m the type of baker who must lick the spoon and sample the finished product as soon as it’s done, so you might assume that this activity makes my blood sugar go up. Not so. And this is because I am also what I call a “frantic baker”. I shuffle around the kitchen, rifle through cabinets, curse when I can’t find an ingredient and need to rush out to the store to get it…now you must get the idea. I’m always in motion when I’m baking, which pays off in the end. I need to try my baked goods in order to boost blood sugar that went low in the process of creating them. This is one of the many reasons why I love baking!
3 – Playing with my puppy. Little Miss Violet is four months old now and more rambunctious than ever. She loves fetching, running, chasing…and nine times out of ten, I’m fetching, running, and chasing right along with her. Before too long, Violet’s winded and on her way to dreamland while I’m on my way to the kitchen to grab something that will treat my low blood sugar.
4 – Cleaning the bathroom. A self-professed neat freak, I have a very specific process when I’m cleaning the 1.5 bathrooms in my condo. This process probably isn’t the most efficient because it involves a lot of walking up and down the stairs to gather various cleaning supplies, but it does do one thing well: lower my blood sugar, of course.
5 – Walking. This is pretty dang obvious because any sort of physical activity/exercise is bound to make my blood sugar drop, but not in the same way that walking does. I swear that 10-15 minutes of walking at a normal pace is enough to drop my blood sugar by about 100 points – that’s how effective it is for me. Walking is my sneaky little trick when my blood sugar is a tad too high: Instead of taking insulin to correct it, I just have to get a quick walk in and I’m falling fast in no time.
Across social media, I keep seeing the same type of photo pop in my feeds that sparks jealousy, triumph, fear, confusion, and hope all at once: the COVID-19 vaccine selfie, fondly referred to as the “vaxxie”.
I’m beyond happy that dozens of family members and friends have received the vaccine. It makes me feel good to know that they’re doing their part to help protect themselves and others, and it’s wonderful to know that the vaccine is being distributed to some extent.
However, I take issue with part of the distribution plan in my state.
Using my voice to hopefully change/improve the rollout of the vaccine in MA felt good.
In Massachusetts, COVID-19 vaccine rollout has been chaotic, to put it mildly.
It’s probably similar in many states, but the part that I find most frustrating is the fact that people with type 1 diabetes (and seemingly no other co-morbidity) are being lumped together with the last group of individuals to be vaccinated.
My endocrinologist confirmed this for me the other day during my virtual appointment: “Why is it [presumably her computer system] showing you in phase 3? You should be in phase 2…” I nodded vigorously and we talked for a few minutes about how disconcerting the whole vaccine rollout plan is. I explained to her that the Massachusetts chapter of #insulin4all was coming up with language to email to local representatives to implore them to do everything possible to prioritize vaccination for all people with diabetes, and a couple days later, I got my chance to do just that.
I looked up my local and state representatives with a quick Google search and emailed three individuals who are in positions to revise public guidance regarding COVID vaccinations. As soon as I hit “send”, I felt this amazing sense of empowerment – it felt good to do something about an issue that I’m very passionate about.
While I wish that I could do more to ensure change, I do feel a sense of pride that I tried to do something by using my voice. It represented the first (but certainly not the last) time that I plan on contacting legislators to help improve diabetes care, management, and accessibility of supplies – not just for myself, but for all people living with diabetes.
My first-ever virtual endocrinologist appointment – and my first one of 2021 – took place last week. I’m going to sum it up list-style, because who doesn’t love a good bullet-point list?
It wasstrange. I didn’t think I would be weirded out by having my endocrinologist “in” my home, but it was freakin’ bizarre to see her face show up on the monitor that I do my day job from, that happens to live on a desk in my bedroom.
I had to wait to see my doctor. It took almost 10 minutes for me to receive my pre-appointment check-in call, and another five before my doctor actually joined. That felt normal.
We made a single change to my pump settings in the whole appointment. She suggested a solitary tweak to my correction factor. I’m not sure I agree with said change, but we’ll see how I feel about it over time.
Look, it’s actually me in the virtual waiting room! Smirking at the camera and everything! Thank goodness my doctor didn’t join at this moment…
My lab results were barely discussed. My doc mentioned that my cholesterol was a little higher than it was last time, and I unabashedly told her that this was probably because I hit the drink somewhat harder than I used to in the past (sorry not sorry, I like wine). I brought up my A1c and I said I was proud of myself for achieving it, and she just nodded, otherwise disregarding this data point.
We figured out which prescriptions I needed. When she asked about my supplies, I explained to her that Dexcom is no longer shipping sensors and transmitters to me directly and they want me to use another supplier called Byram (more on that in a future post). I asked if she could send my prescription to my regular mail-order pharmacy instead, and she obliged, telling me to double-check on the script in a few days to make sure it would go through properly.
It was just as short as they typically are. The whole damn appointment lasted only 15 minutes and 2 seconds…and we talked about me/my diabetes, specifically, for fewer than 5 minutes. We spent the rest of the time discussing our collective confusion over my COVID vaccine eligibility and my frustration over my postponed physical. It was both gratifying and dismaying to discover that she couldn’t understand why the state of Massachusetts considers me ineligible to receive the vaccine until the third (final) distribution phase, but I’m hoping that will change soon.
She wants to see me again in 6-7 months. My doctor ended the appointment by asking me to schedule an appointment in the August/September range, which seems so far away. I let her know I’d schedule it at a later date for a couple of reasons, one being that I have no clue whether I’ll want to go in person or do it virtually again, and another being that I really don’t know that I want to keep her as my endo.
That just about covers it. I’m not the happiest patient in the world – I’ve been uncertain about this doctor since I started seeing her – but for realsies, I’m glad that I trusted my instincts and requested a virtual appointment instead of an in-person one.
The drive would’ve been longer than the visit, and for me, that just doesn’t make it worth it.
I literally just got off the phone with OmniPod/Insulet as I’m writing this post.
I jumped on the computer right away because I was so impressed with the speediness of their customer support team.
Normally, I only call customer support to report the occasional pod failure. I had my first one of the year over the weekend, so I made some time during the week to give them a call and tell them about it.
I’m used to being hit with all kinds of questions when I call customer support: Where were you wearing the pod? What were you doing when it failed? How long were you wearing it for? What kind of insulin were you using in it? What’s your date of birth/shipping address/Social Security Number? (Okay, they don’t ask about that last one, but they need so much information from me that they might as well get that, too!)
This time, after I verified my shipping address, I was simply asked to rattle off the alarm code that triggered this pod failure, and state approximately how long I wore the pod.
That’s it.
I couldn’t believe how quick and easy it was to get a replacement pod.
Just a couple easy questions that I could answer straightaway because I had my PDM on hand (I always do when calling Insulet because 9 times out of 10, they’ll need information from it). The rep I spoke to on the phone just had one final question for me: Did I mind ground shipping for the replacement they were going to send to me, or did I need them to overnight it?
I let her know that standard shipping was just fine, and then I felt compelled to tell her that I was appreciative of her swift solution and professionalism. She thanked me and also clued me into the fact that Insulet’s worked hard to streamline the number and type of questions asked when customers call in, which made someone like me doubly happy.
I thanked her for her help again before hanging up the phone. Then I noticed: The length of our phone call was just under 5 minutes. It takes me a bit longer than that, on average, to apply a new pod.
In 5 minutes flat, a replacement pod was on its way to this satisfied customer. It’s nice to know that when pod failures happen – they do, and they will happen again – it’ll be much easier going forward to get them replaced.
One of the many reasons why I love the diabetes community is that I’m constantly learning new information, finding inspiration, and enjoying support from my fellow friends living with T1D. Sharing our stories with one another leads to us finding that it’s more than diabetes that we have in common.
Here’s an example: My friend, Cherise Shockley, recently wrote an article for DiaTribe in which she made a confession to herself regarding how she counts her carbs. I recommend reading the extremely well-written article to get a full sense of what she discovered, but in short, Cherise recently realized that her carb counting is inaccurate because of the “glass ceiling” for entering carbs into her pump for bolus calculations. In other words, Cherise’s personal maximum of carbs that she was comfortable with dosing for using her pump wasn’t aligning with the actual amount of carbs she was consuming. This excerpt explains part of it:
That was my moment of truth. I told Natalie I ate my favorite chocolate chunk cookie that day. She asked me how many carbs the cookie contained, and I told her 68 grams; she wondered why I only bolused for 55 grams. I paused before I replied – I did not know the answer.
Natalie then asked me if I had a glass ceiling for entering carbs in my pump. She explained that this means even though I know I eat 63 carbs, I will only enter 50 carbs in my pump because anything higher than that concerns me. What she said was interesting; I had never heard anyone describe it to me in that way.
-Cherise Shockley
When I read this, I said, “Yes! Finally, someone is able to articulate exactly how I handle carb counting!”
This is the truth about my carb counting: I have limits when it comes to how many carbs I will bolus for at a time, but those limits do not apply to the actual number of carbs that I consume.
In my 23 years of life with type 1 diabetes, I never knew the meaning behind my carbohydrate glass ceiling.
To explain, I am only comfortable with bolusing for a maximum of 60 grams of carbohydrate at a time. I do not know how I came up with this particular number, but I do know that there are situations (e.g., holiday celebrations) in which I am absolutely consuming more than 60 carbs in a sitting, and yet I only bolus for that amount.
Still confused by what I mean? Read the full article to understand, but this excerpt from it helps to explain why this fear of bolusing for more than 60 carbs at a time exists for me:
To learn more about carbohydrate glass ceilings and why some people have one, I talked to Dr. Korey Hood, a professor of pediatric endocrinology and psychiatry and behavioral sciences at Stanford University who has lived with type 1 diabetes for over 20 years. Dr. Hood told me that all parts of diabetes management can be challenging, and carb counting is particularly tough because it is hard to be accurate and precise. He always recommends people with diabetes meet annually with their diabetes educator (CDCES) to get a refresher on different aspects of diabetes management, including carb counting.
Dr. Hood said that the glass ceiling is most likely due to one of two issues – worries about hypoglycemia or the meaning behind taking such a big dose of insulin. Dr. Hood said that “many of us with diabetes, particularly those on insulin, worry about going low. Why wouldn’t we – it is a terrible feeling! We often experience fears of hypoglycemia because we had a terrible low in the past and have a desperate desire to avoid it in the future. When we worry about hypoglycemia, we scale back our insulin dosing. This prevents the low but also likely results in high glucose levels. So, it really is not a good strategy.”
-Cherise Shockley
This was a major revelation for me because suddenly I realized what my reasoning is for my carbohydrate glass ceiling: I have a hypoglycemia fear. I have experienced scary episodes in the past (fortunately, none of which have required medical attention). I have friends who have experienced severe hypoglycemic episodes, and when a colleague of mine experienced a low episode that was so bad that I had to call 911 for him, it left a mark on me. So on the occasions that I do eat more than 60 carbs in a sitting, I simply don’t take the amount of insulin that I should to account for those carbs, and I wind up going high, exactly as Dr. Hood describes in the quote above.
When it comes to diabetes, there is no such thing as “perfection”. My blood sugars cannot and will not be perfect 100% of the time. But one thing that I do have control over is doing the absolute best that I can with carb counting and bolusing. It’s time I hold myself more accountable to my carbohydrate glass ceiling…in fact, it’s time for me to smash through it.
A ginormous thank you to Cherise for being so open and honest in this piece and for inspiring me to own my carbs, too.
I’ve been writing blog posts for Hugging the Cactus for just over three years now. In that span of time, I’ve accumulated more than 500 posts total, and I don’t plan on slowing down any time soon.
Obviously, though, some of those posts have been more popular than others. I thought I’d link to them all here because 1) it’ll be helpful for both my readers and to me to see which topics garner the most interest, and 2) it makes for easy clicking to get to the top articles! So without further ado…
The only thing missing from my blogging location is…a real cacti. I got plenty of fake ones, though!!
Is a Bleeder a Reader? My Take on a Bloody Dexcom G6 Insertion – This is the top blog post of all time (so far) here at Hugging the Cactus. It’s got more than 6,000 views and proves to me that many people who use Dexcom sensors aren’t sure whether bloody sensors indicate an inability to measure blood sugar readings. If you aren’t sure yourself, click the link for my take.
My One-Month Dexcom G6 Review – People seem to dig reviews (I know I love reading product reviews online), so it’s pretty obvious why this comes in third place. Plus, I wrote it early on in the release of the Dexcom G6: Due to my participation in the advertising campaigns, I was lucky enough to be among the first individuals in the country to start using the G6.
T1D and Cosmetics: My Thoughts on Jeffree Star’s “Blood Sugar” Palette – I can only guess that this one is a high performer because Jeffree Star is the kind of character who gets a lot of attention online. Still unsure why he named an eye shadow palette “blood sugar” (tacky IMO), but whatever.
That “Thing” on my Arm – What is “that thing” on my arm? Is it a large nicotine patch? A weird new piece of statement jewelry? Or something else? In this blog post, I write about a situation in which I was asked about the “thing” on my arm and how I handled it.
Insulin Pumps and X-rays – I didn’t realize I had no clue what the protocol is when it comes to insulin pumps and X-rays until I actually had a broken bone! It taught me a lesson that I won’t forget about whether or not it’s safe to wear an insulin pump when getting an X-ray.
Restarting the Dexcom G6: Attempt #2 – The Dexcom G6 wasn’t out for long when the diabetes online community started hacking it to figure out whether or not it could be restarted and worn for a longer period, just like its predecessor. It took me a couple of tries, but I finally found a method that sorta works, as described in this post.
How Long Do OmniPods Really Last? – In this blog post, I reveal the true life cycle of an OmniPod…did you already know this, or was this new information to you?
The CGM Experiment: Comparing the Dexcom G5 to the G6 – I remember that people were verrrrry curious about the differences between the Dexcom G5 and the G6 when the G6 debuted. Could it really put a stop to fingerstick checks? Was it more accurate? Was it painless? I compared the two in this post and, hopefully, answered a lot of questions that people might have had about how the G6 measures up to the G5.
The Best (and Worst) Insulin Pump Infusion and CGM Sensor Sites – I shared my opinions in this post on what makes the best and worst sites for my medical devices. If anyone is wondering about trying a new site, chances are I’ve described how I feel about it in this post.
It’ll be interesting to see how this top 10 list changes in the coming months and years. One thing is for certain, though: I’ll continue to do my best to deliver engaging content that is truly helpful or supportive to our diabetes community. It’s my honor to contribute in any way that I can.
“Molly, we’re calling to inform you that your 10 A.M. appointment for this Thursday has been canceled. We still aren’t taking patients in the office and we won’t be rescheduling you until April. Please give us a call back so we can set up a new appointment time.”
I listened to the voicemail twice before it sank in that my primary care doctor’s office was calling me to postpone my annual physical.
Why, exactly, did it get postponed? And how do I feel about it?
My doctor’s office called me two days before I was scheduled to come in…leaving me to also wonder why such short notice of the cancellation?
Well, I can only theorize the answer to the first question. I’m certain that my doctor’s office is absolutely overwhelmed with phone calls and appointments…and they’ve probably been like that for the past year or so. I’m guessing that they’re only keeping appointments with higher-priority patients that absolutely need to be seen…someone like me, a pretty healthy (discounting my diabetes) and younger individual, is likely not very high on the list of patients they want to see. Plus, even though I know they’re doing virtual appointments for medical questions as they come up, there probably is no purpose in doing a virtual physical because there’s only so much they can do via video call. So I get the postponement, but that doesn’t mean I’m happy about it.
My annual physical is the doctor’s appointment for me, the one that I have each year that I know won’t be a total waste of time. Each year, I get my blood work and urinalysis completed at this appointment, as well as an EKG to monitor my heart. I also get to go over any general health concerns I have with my PCP, who is very thorough when explaining things to me. During this particular visit, I’d hoped to talk about (what I believe to be) the stress-induced hives I’ve experienced in the last month, but now it sounds like I won’t have the chance to do that until April.
But I’m also wondering…when I go to the appointment in April, will I receive my COVID vaccine then, too?
I messaged the doctor’s office to find out and learned…nothing helpful:
I believe by that time you should qualify for the vaccine so you should be able to get it. This of course depends on if the state has given us the vaccine. We will know soon about that and will be sending information to all our patients.
Uhh…according to the multi-phase vaccine plan outlined by the state of Massachusetts, I should be eligible for the vaccine prior to April. (But quite frankly, the whole phase plan has been a bit of a hot mess. I’m just glad to have 2 out of 4 immediate family members vaccinated at this point.) And the “if” there? Definitely unsettling.
I have so many questions: Can they postpone again in April? When will they be able to tell us more information about the vaccine? Do they think that it’s safer to wait in April because there will hopefully be more vaccinated individuals overall then? Or are they actually worried about vaccine distribution and don’t want to clue anyone into that?
So I feel not-so-awesome about having to wait three more months to check in with my PCP. I take my overall health very seriously, not just my diabetes. One thing has everything to do with the other. However, I do have a virtual appointment with my endocrinologist in a few weeks…maybe that will be the health check-in that I’m desiring?
This time last year, I was under the impression that I’d be heading to the Friends for Life Orlando conference that is held each July.
It was supposed to be my “triumphant return” to in-real-life diabetes meet-ups. There were so many individuals I’d hoped to either reunite with or meet for the first time.
Obviously, the pandemic totally changed my plans – as well as everyone else’s.
I was upset for awhile, but took consolation in the fact that the FFL team worked hard to turn it into a virtual conference. IMHO, I think they did an excellent job, and I remember signing off from that one feeling hopeful to attend it in-person in 2021…
This time last year was supposed to go a little differently.
…except I just don’t think that’s going to happen for me this year.
As far as I’m aware, the CWD FFL Orlando conference is on and in-person for 2021. But I, personally, am not comfortable attending. I know this won’t be the case for everyone and that’s okay. Yet I still feel compelled to explain why I’m not going to attend and how this makes me feel.
I don’t feel good about traveling, well, anywhere these days. I have a lot of anxiety about it, so much that any type of getaway, as nice as it sounds right now, just wouldn’t be worth it in the end because of how much worry I’d have about the trip.
And of course I’m sad about this. Of course I want to escape somewhere, and OF COURSE I’d love the chance to see my diabetes community in person. I find that in-person interactions are so much richer and fill me with a sense of gratitude and camaraderie that just can’t be matched online. Plus, I feel that it’s much easier to forge genuine connections when interacting with others face-to-face…I struggle to keep up with all the tweets, Instagram posts/stories, and Facebook threads, so instead of trying to weed my way through them all, I typically just don’t engage whatsoever. I simply can’t find enough time to comment as much as I’d like, which means that I miss out on some great opportunities to satisfy my need for conversation with the diabetes community.
As much as my decision not to attend bums me out, I do take some solace in knowing that there are others in the same boat as me. And I also feel reassured thinking about how hopefully, this time next year, I will be planning my true comeback to the wonderful world of diabetes conferences (in the wonderful world of Walt Disney, to boot).
I have a new favorite breakfast, both blood-sugar-wise and taste-wise, that I just had to write about here.
And that breakfast is: egg wraps! I take a low-carb spinach and herb tortilla, add eggs, sprinkle on some cheese, tuck in some turkey sausage or a scoop of guacamole, and wrap it all up for a totally delicious, lower-carb meal that I honestly can’t get enough of these days.
I love how surprisingly versatile this breakfast wrap is. I can lighten it by using scrambled egg whites in place of eggs with yolks, I can season it however I want (though my preference is everything but the bagel seasoning), and when I’m feeling spicy, I can add a few shakes of garlicky hot sauce for some zip. When I have fresh veggies, I’ll add those to the wrap, too, for some more color, flavor, and texture. Sprouts are really great in this kind of wrap, as is spinach or even chopped onions and peppers (I like cooking frozen ones with my eggs because they’re easy to have on hand at all times).
You’re probably wondering why I didn’t take a picture of my wonderful wraps for this posts and well…I ain’t a food blogger, I take awful food pictures! So just pretend this photo is a perfect representation of my new fave breakfast. Please and thanks. 🙂
So obviously this wrap is a winner in terms of taste, but it’s really excellent for my blood sugars, too. I don’t typically bolus for more than 15 carbs for this meal (the wrap is only 4 net carbs and everything else that I add in has negligible carb content OR I just bolus for the protein) and the low glycemic index means that I never see a blood sugar spike after eating one of my wraps. And let me be real: I love my breakfast carbs (waffles, pancakes, muffins, even cereal…omg they’re all amazing to me), but they’re a pain in the ass to bolus for properly. Even when I do nail my bolus for a high-carb breakfast item, I’m not always able to do a pre-bolus (in other words, take insulin 15-20 minutes before I eat to give it time to start working ahead of the carbs) and avoid that carb-induced spike…which means I end up skyrocketing shortly after I eat, only to level out later. That’s not the worst thing in the world, but I’d prefer to not experience any sudden blood sugar jump, period.
Need I sell the benefits of this breakfast any further?! Knowing myself, I’ll have a new morning staple before too long, but for now I’ll *wrap* up this blog post on my *eggs*cellent breakfast wrap before I get too *cheesy* with the puns…