What a strange sentence to write, since oftentimes I feel that I am simultaneously much younger and much older than 30. I’ve got a childish sense of humor and a penchant for video games and shirking responsibilities, but I also quite enjoy going to bed early and have my fair share of aches and pains that I complain about almost daily. But in reality, I’m merely entering my third decade of life, and taking my 25 years of diabetes (so far) along with me.
I’m also bringing the following mantra into my thirties: The best is yet to come. That’s because I have an unshaking faith in knowing that I’ll make many of my goals, hopes, and dreams turn into a reality in this decade – I will manifest them into existence, dammit, if that’s what it takes.
In addition to my excitement over this realization, it’s also beginning to dawn on me that this attitude can apply more specifically to my life with diabetes. I’ve seen for myself in the last 25 years just how far we’ve come, in terms of everything from standards of care to technology. How can I not have confidence, then, in the belief that the best is yet to come for myself and all other people living with diabetes? I can say with utmost certainty that the technology will only continue to get better, accessibility barriers will continue to be broken down, affordability will continue to improve, and my own diabetes care and treatment will continue to adapt and advance as time goes on.
So today, rather than mourning the end of my roaring 20s, I’m welcoming my 30s with open arms and the expectation (to riff on the movie 13 Going on 30, in which turning 30 means that one will be 30, flirty, and thriving) that they will be marked by a period of thriving with the knowledge that the best truly is yet to come.
This blog post was originally published on February 9, 2019, on Hugging the Cactus. I’m sharing it again today because it’s a great reminder that trying new things (in terms of both diabetes and life in general) can be scary but definitely worth it. Oh, and that I have a really great dad. Read on for more…
The first time I self-injected insulin, I was absolutely terrified at the mere thought of it.
Since I’ve never really minded needles that much, you’d think that self-injecting would be a cinch for me. That couldn’t be further from the truth, at least for the first few times that I had to do it.
It goes back to one endocrinologist appointment when I was nine, maybe ten years old. My doctor and my parents were talking about how I was reaching an age where I should start to take on a little bit more responsibility in terms of my diabetes care. I don’t remember whether my endo or my parents suggested it, but one of the two parties said that a good starting place would be to start giving myself my own insulin.
Initially, I protested. I hated the idea. But I warmed up to it when my parents reassured me that they would check the syringe for me before I stuck it into my skin. At this point in time, I’d practiced drawing up my own insulin dosages. I’d pass the syringe along to my mother or father for the actual injection. So I had the first step in the process down pat, and it only made sense for me to put two and two together and do it all independently.
Since I was hemming and hawing over the prospect, though, my endo had the brilliant idea to practice on my father with a saline injection right then and there, given that he was willing for me to do it. As he rolled up his sleeve, I grinned wickedly (I was annoyed with him for some trivial reason that day) and waited while my doctor prepared the saline injection. As she brought it over, I panicked a little, and I must’ve asked two or three times whether it was actually safe for me to do this. Because even if I was irritated with him, for whatever stupid thing it was, I didn’t actually want to hurt him.
Once I was adequately assured that the injection would be harmless, I took the syringe into my hand, took a deep breath, and stuck it into my dad’s arm. I remember pushing down on the plunger slowly, and my dad sitting in the chair, totally composed and un-bothered by the sensation. When I took the needle out of his arm, I exhaled loudly, not realizing that I had been holding my breath the whole time. What can I say, it was a nerve-wracking feeling. It’s not every day that you learn how to inject yourself, or someone else for that matter, with a syringe.
Over the course of the next week or two, I practiced my new skill on oranges supplied to me courtesy of my parents. With each practice injection, my confidence grew and I realized that it wasn’t that scary. I would press the orange against my leg or my arm, pinch at its peel, and give it an injection of salt water – super quick, super easy.
In no time at all, I felt brave enough to give myself my first self-injection. Just like I did with my dad in the doctor’s office, I breathed deeply before plunging it into my leg, exhaling only when I was done. And I felt the satisfaction of having done it on my own, which was sweeter than I thought it would be.
Working up the courage to self-inject is just one example of many experiences I’ve had with diabetes and being afraid to try something new. Whether it was trying a CGM for the first time or transitioning to a pump, each new thing I introduced to my diabetes care and management routine scared the hell out of me at first. But just like I proved to myself that self-injecting was nothing to be afraid of, I’ve shown myself time and time again that new things for diabetes aren’t always so bad.
This blog post was originally published on Hugging the Cactus onMarch 7, 2022. I’m sharing it again today because I (and other people with diabetes) constantly battle the misconception that I can’t eat foods that contain sugar/carbohydrates. Why, just the other day, someone who has known me since I was 12 years old made a comment about how I couldn’t eat cookies! In that situation, I smiled politely and gently corrected the individual, but the bottom line remains: This is some diabetes stigma that I’d like to defeat. Read on for more…
Yes, I have diabetes.
Yes, I can eat cheesecake and pizza.
Yes, I can actually eat whatever I want – I just have to know the carbohydrate content of whatever I’m consuming (and being mindful of portion size doesn’t hurt either).
Yes, I’m telling you this because at the time of this writing, that’s actually what I had for lunch this afternoon: homemade pizza and cheesecake. The pizza crust was store-bought, but everything else – from the sauce to the cheesecake crust to the strawberry topping – was made by me and it was damn good.
I guess I’m just taking a moment to 1) congratulate myself on semi-mastering the home-cooked versions of these two foods, but also to 2) reflect on how there’s so much stigma, STILL, on what people with diabetes can/can’t or should/shouldn’t eat. It’s wild to me that there are countless people in our world who misunderstand that a diabetes diagnosis automatically eliminates certain food groups from an individual’s diet.
Let me say it louder for those in the back who can’t hear: People with diabetes can eat whatever they want. Diabetes varies from person to person, and so do dietary preferences – so just because one person with diabetes might follow a strict keto diet, it doesn’t mean that ALL people with diabetes do. It doesn’t make it right or wrong for a person with diabetes to choose or not choose to eat certain things – period, bottom line, end of the story.
And by the way – I took a big old bolus of insulin for aforementioned pizza and insulin and my blood sugar didn’t spike past 188 mg/dL several hours later – score! So I’m also using this blog post to remind myself that it’s okay to eat “treat” foods like this from time to time, and that does not make me a bad diabetic.
If you aren’t familiar with the acronym AITA, then let me break it down for you: It stands for “am I the asshole”?
It stems from Reddit, which is basically a ginormous discussion thread website. It provides a forum for people to post stories in which they’re unsure whether they’ve acted like, well, an asshole. Then other folks who see the initial post can chime in with their opinion on whether they think yes, the OP (original poster) did act selfishly/foolishly/asshole-ly or no, the OP acted in accordance with what they would have done, had they been in that person’s shoes. It can be a wildly entertaining guilty pleasure to fall down the rabbit hole of these discussion threads and deduce for oneself if a perfect stranger on the Internet did indeed act like an asshole in a given situation or not.
I found myself immersed in one of these AITA threads that my cousin sent me because, of course, it had to do with diabetes. Long story short, the OP wondered AITA for moving their roommate’s insulin out of the way, causing said roommate to panic and be forced to resort to an emergency insulin supply because they were unable to locate what had been stored in the refrigerator. Now, in just that context alone, I would’ve said that the OP wasn’t an a-hole because they probably just didn’t know any better, but as I scrolled further along in the thread I discovered that they thought it was fine to do and that diabetics were fine in historical times when there was no refrigeration. And he took his ignorance a step further by posting a comment about how he didn’t know what the big deal was about taking a vial of “sugar water” – yes, that’s what he called insulin – out of the fridge.
That’s when I immediately realized, yep, the OP can wear the AITA crown with certainty. This whole anecdote might come across as a teensy weensy blip in the universe of Internet discussion threads, but to me, it stands out as a perfect example that even people who are closest to those living with T1D can get such a significant detail about it so, incredibly wrong. And it’s proof that we’ve got a long way to go in terms of educating the world on the importance and purpose of insulin, apparently, even though stories about it have hit so many headlines in recent years.
TL;DR (another Reddit acronym meaning too long; didn’t read): Let’s get it straight, now, that insulin is a life-saving medication that needs to be stored properly in order for it to be used – and IMHO (in my humble opinion), never take it away from a person living with diabetes without asking them about it first.
Any type of pizza, plus diabetes, usually equals one giant headache in terms of nailing a correct insulin dosage.
Nine times out of ten, my blood sugar ends up high in the hours following a pizza meal. This is a fairly common phenomenon for people with diabetes, because even though pizza contains high amounts of carbohydrates, it also contains a large amount of fat that ends up delaying the digestion of pizza – resulting in a belated blood sugar spike. My go-to workaround for this is to do an extended insulin bolus, meaning that I take part of my insulin dose at mealtime and my pump will deliver the remaining dose later on, but it can be tricky to nail the timing of it.
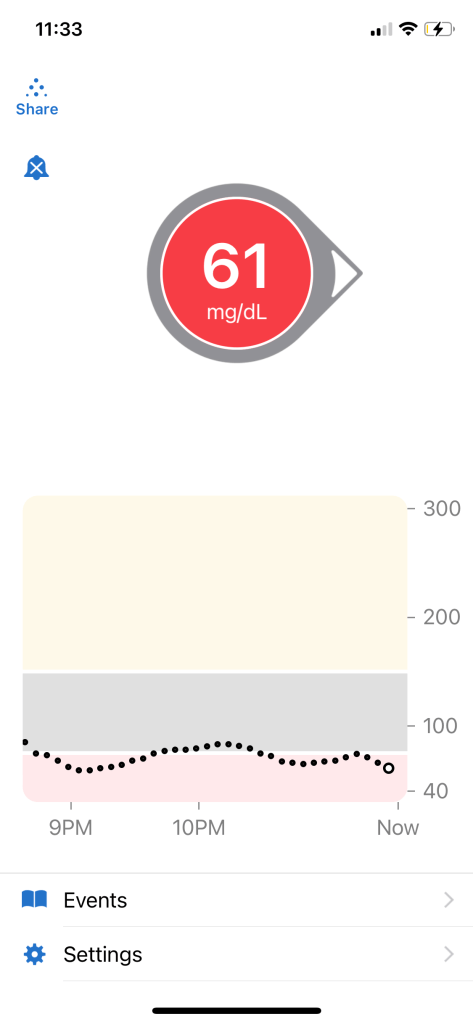
So imagine my surprise when, after enjoying an evening out with my boyfriend in which we split a very tasty flatbread pizza (half buffalo chicken, half brussels sprouts and bacon), my blood sugar didn’t spike even a little bit post-meal. In fact, it actually ended up tanking – so much so that over the course of 2 hours, I had to eat 3 packs of fruit snacks and a handful of leftover Easter candies in order to keep it from dropping too much.
My mind was blown. I had actually eaten more flatbread slices than I normally do during this meal – the two of us nearly demolished a large-size flatbread, which is quite a feat – and so I bolused for 60 grams of carbs, using the manual mode on my Omnipod 5 PDM to enable an extended bolus in which I gave myself half my insulin dose upfront with the remaining half to follow 1 hour later. I actually thought I was underestimating the total carbs I’d consumed, especially considering I had two cocktails with my meal. But nope, I had completely missed the mark on this one and paid the price as I did whatever I could to keep my blood sugar up in the hours before I planned to go to bed. You can see from my CGM graph below that this was a bit of a prolonged struggle, one that kept me up much later than I would’ve liked.
But, oh well. That’s just how it is with diabetes sometimes, and I remain optimistic that I can nail the pizza bolus next time. After all, I’ve done it before, so I can do it again. And this is the kind of bolus experiment that’s kind of enjoyable – any excuse to have some delicious pizza.
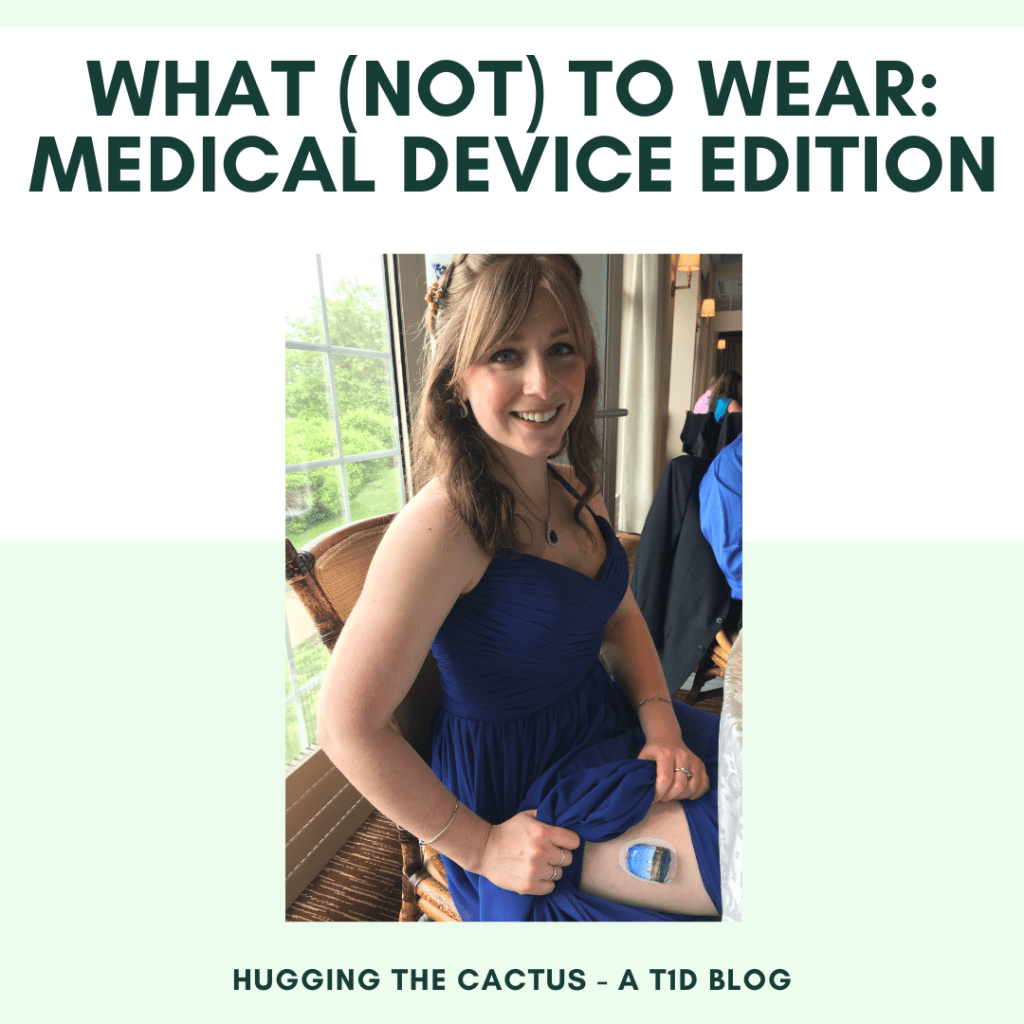
I’m going to two weddings this spring and summer and rather than stressing about which dress I’ll wear to each, I’m finding myself more focused on where I’ll wear my insulin pump and my CGM.
It might sound like I’m making a mountain out of a molehill, but truly, I’m having a hard time deciding whether or not I want to make an effort to hide my devices or don them proudly along with my formalwear. Now when I say “hide”, I don’t mean that I want them out of sight because I’m ashamed of them or anything negative like that. It couldn’t be further from the truth. I’m proud of and grateful for my pump and CGM, but that doesn’t mean that I want them to be front and center on a special occasion. I’d rather let my style – my dress, my make-up, and my jewelry – shine because they’re more reflective of who I am as a person. My diabetes is also a part of my identity, but I don’t want to showcase it if it can be avoided. I also don’t want to attract stares, because whether I like it or not, people will always look and wonder what my pod and CGM are and why I have to wear them.
At a family wedding a few years ago, I was proud to showcase my cute pod sticker…but these days, I’m not so sure that I want to go about advertising my diabetes so boldly at a couple of upcoming weddings!
So based on that logic alone, I’m leaning towards wearing my pod and CGM on sites around my abdomen or legs, keeping them neatly tucked away underneath my wedding attire. But I also need to take into account my site change days. My pod is changed every 3 days, and my CGM sensor is replaced every 10 days. I could plan backwards from the wedding dates and figure out where I need to place my pod and sensor according to that, but let’s be real here: I don’t always have the mental bandwidth to plan that far in advance. Pod and sensor site changes are so routine to me at this point that I just kind of go through the motions every time that I change them, and don’t give much thought to their particular placement beyond making sure that I’m properly rotating my sites. Maybe I’m just being lazy by claiming it’s too much extra work, but honestly, there’s so much work that already goes into diabetes on a daily basis that I just don’t want to give in and plan out a site change timeline that guarantees covered-up diabetes devices.
We’ll see what happens, but one thing is for sure: Whether I showcase my sensor and pod in visible spots or if I choose to keep them covered up, I won’t let my diabetes spoil any aspect of having a great time celebrating at both weddings.
“Bolus-worthy” is a term that, I believe, is semi-universally used by the diabetes community to describe food/drink that’s worth taking insulin for. Not just any typical amount of insulin, though – usually something that meets bolus-worthy criteria is something that requires extra insulin, and probably a little bit of guesswork, too.
What makes something “bolus-worthy”? And is it always truly worth it, even if it produces less-than-desirable blood sugar outcomes? I’ll attempt to answer both of these questions from my own unique point-of-view.
I think that a food or beverage is bolus-worthy when it’s something that I can’t and won’t indulge in often. It’s important to consider the “and” between those statements because it must meet both of those conditions; otherwise, it’s simply not special enough to be considered bolus-worthy. So something like the slice of carrot cake that my mom and I shared on our annual outing to a local teashop was totally worth taking extra insulin for, whereas pretty much anything I could order from a McDonald’s menu isn’t (I only ever go to fast food restaurants as last resort, and it doesn’t make me feel particularly good to eat food like that often). I believe in allowing myself carb-laden foods – ice cream, pizza, desserts from a bakery, you name it – whenever the desire strikes, but I do try to be careful about making sure I don’t do that often so that way I can have a better handle on my blood sugar levels as well as make myself more likely to really enjoy the indulgence.
But just because something fits into my “bolus-worthy” definition, is it always worth potentially paying the price of having a blood sugar I’m unhappy with later on? It depends. On an occasion like my birthday, I like to pretend that any out-of-control blood sugar levels don’t count as I eat whatever celebratory goodies I like – even though I’m subconsciously aware that of course they do, and TBH I actually prefer to stay in-range on my birthday so that my diabetes can’t steal the day from me. I guess this is kind of the beauty of the “bolus-worthy” label, though. To me, it implies that whatever it is that I’m having is reserved for special moments. That in itself makes anything worth it, if it’s contributing to the meaning behind an occasion.
And I look forward to putting this theory of mine in action on my birthday in a few short weeks, a time that I guarantee will be filled with food and drink that I deem 100% certifiably bolus-worthy!
I feel like the luckiest person with diabetes in the world – not because I have diabetes, but because diabetes has made me grateful for many things in life; mainly, my support network.
I’ve had two very minor health scares this month (one being my bout with the stomach bug and the other being a scary middle-of-the-night low blood sugar), and in hindsight, it’s embarrassing to think about how worked up I got over both of these incidents. But I’d be remiss if I didn’t recognize the people who helped me get through these events and didn’t judge me whatsoever for the anxiety that, at those moments in time, I struggled to reign in.
My parents and my partner listened patiently and offered advice each time. They didn’t hesitate to offer to run to the store to get me anything that I needed, nor did they complain when I called late at night to let them know what I was experiencing. Fortunately, I don’t always need this level of support (especially when it comes to dealing with a low), but that doesn’t make me any less appreciative of the fact that they showed up for me when I was feeling particularly panicky, heightened by being alone.
And that’s what makes me the luckiest – the knowledge that I’ve got the best allies in my corner who are there for me when I’m strong as well as vulnerable.
This blog post was originally published on Hugging the Cactus on April 12, 2021. I’m sharing it again, ahead of the Easter holiday, as a reminder to myself and others that it’s perfectly okay for people with diabetes to indulge in sweets – just like everyone else, though, it’s important to do so mindfully. Read on for my tips…
If you regularly read this blog, then you know that I’m not a strict person with diabetes, in the sense that I don’t really restrict the foods that I include in my diet.
I’ve always been of the mindset that my diabetes can’t dictate what I choose to consume, though it might limit the actual quantity of a given food type that I eat.
So while my fridge and freezer is almost always stocked with fresh and frozen fruits/veggies/proteins, my pantry often stores more shelf-stable (and usually less healthy) things like crackers, cookies, and even candy. In fact, a full week post-Easter, my cabinets contain 3 bags of jellybeans, a chocolate bunny, and several Reese’s eggs. And it’s very tempting to reach into the cupboards and help myself to as much sugary sweetness as I can stomach in one sitting – screw my diabetes/blood sugar, I’ve got delectable confections to consume!
But of course, I know that indulging my cravings will only wreak havoc on my blood sugar levels, so I’ve found a few ways to curb temptation but still keep tasty treats in my home. Here’s 4 things that have worked for me:
Only eat these treats when my blood sugar is low. I call this “medically necessary” candy consumption, and let me tell you, it makes low blood sugars a whole lot more tolerable when they’re treated with something that’s more fun and yummier than chalky glucose tablets or juice boxes.
Keep them out of sight. I do my best to shove bags of treats in the very back of my top cabinets. That way, if I’m tempted to dig into them, I remember that I won’t be able to reach them unless I get a chair and rummage through the contents of the top shelves…and usually, that’s enough to take away my desire to snack on something sugary. I’m not saying it always happens, but laziness will typically beat my sweet tooth.
Pre-portion single servings of treats. I have a real problem with snacks that come in bottomless bags – it’s hard to know when to stop and my blood sugar always suffers the consequences. So I like to study the serving size on bags and use it as a guide to portion out single servings of treats. It’s much easier to bolus for whatever it may be (or treat a low blood sugar as described in tip #1) when I know the exact carbohydrate count; after all, a few handfuls of an unknown number of Skittles have far more carbs than a single serving of 15 Skittles.
Be picky about the types of treats kept in the house. My kryptonite is most definitely Reese’s cups…I love the salty/sweet combination of peanut butter and chocolate almost as much as I love my dog. So I recognized that a bad habit was forming when I kept a little bowl out in my living room filled to the brim with mini cups. I was breaking every single one of the above rules with this practice! After I realized this, I put the bowl away and stopped buying Reese’s every time I went to the grocery store. I still have other things around the house that will satisfy my sweet tooth (before Easter, I bought a package of dark chocolate Oreos that I’ve easily kept around for the last 6 weeks because they don’t tempt me in the same way that Reese’s cups do), so I’m really not depriving myself at all.
Temptation can be tricky to navigate when you have T1Ds and love sugary treats as much as I do…but as long as you can come up with ways to cope with temptation like I did, then you don’t have to feel guilty for giving in to your cravings every now and then. I sure don’t!
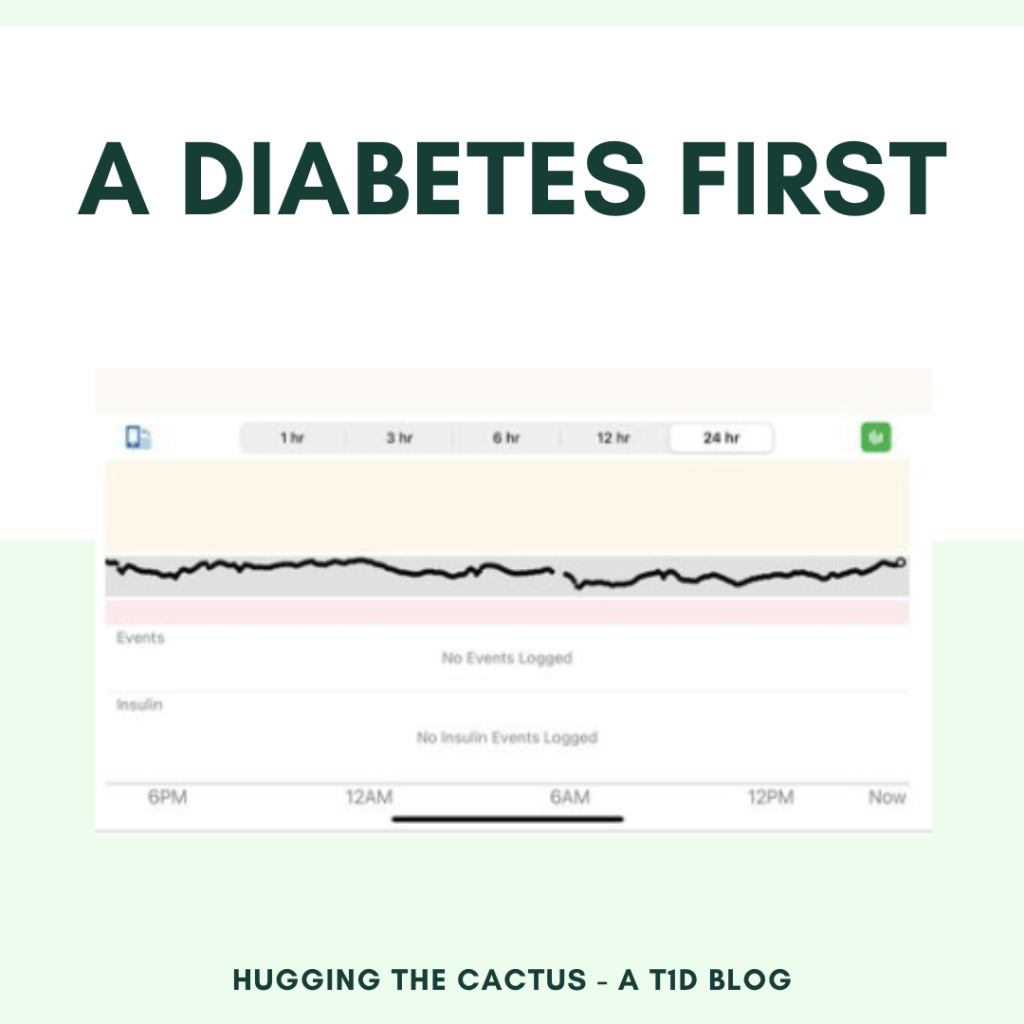
Forget “a diabetes first” as the title for this blog post – “a first” would suffice. That’s because I experienced *drumroll please* my very first stomach bug this past weekend! (At least, the first one that I can remember; most certainly, the first of my adulthood.)
I don’t know how I caught it and honestly, as I sit here and write this, it’s taking the very little energy I have to summarize what I dealt with over the weekend. But here’s the short version: I was out shopping with my partner on Friday evening. On our drive home, I grew increasingly nauseous and essentially bolted it to the bathroom when we made it home. I won’t cover all the gory details here, but basically, I was pretty ill for many hours. Food and drink quickly became out of the question for me, and even though my stomach was churning relentlessly, I still had enough mental bandwidth to check my blood sugar every so often to make sure it wasn’t climbing or falling.
Much to my relief, my blood sugar was the only thing that remained stable all weekend long. As I fought through waves of nausea, I was grateful that I didn’t have any insulin on board as an additional factor to contend with. It seemed like my diabetes knew I was going through enough, so the least it could do was play nice while my body dealt with the bug as best as it could.
I’ve slowly reintroduced foods into my diet today – I never would’ve thought I’d be so simultaneously excited and nervous to eat saltine crackers, rice, or plain chicken – and I’m still amazed at how my diabetes seems to be cooperating as I continue to recover. Granted, this could be because I’m eating very simple carbohydrates and not many at one time, but still. I’m appreciative of the fact that I can rest up without worrying as much about my blood sugar levels.
Don’t get me wrong, though…as nice as it was to have approximately 48 hours of in-range blood sugars (above 80 and below 150 on my own Dexcom graph), I definitely wouldn’t trade them in favor for a stomach bug. I’d much rather put in a little more effort on my own to obtain in-range readings than have to go through that whole ordeal again.