Yes, I can actually eat whatever I want – I just have to know the carbohydrate content of whatever I’m consuming (and being mindful of portion size doesn’t hurt either).
Yes, I’m telling you this because at the time of this writing, that’s actually what I had for lunch this afternoon: homemade pizza and cheesecake. The pizza crust was store-bought, but everything else – from the sauce to the cheesecake crust to the strawberry topping – was made by me and it was damn good.
Funny story: I sent a picture of my cheesecake (shown above) to my coworkers and because I have terrible lighting/I’m not a food blogger, someone thought it was a photo of baked beans and I couldn’t stop laughing.
I guess I’m just taking a moment to 1) congratulate myself on semi-mastering the home-cooked versions of these two foods, but also to 2) reflect on how there’s so much stigma, STILL, on what people with diabetes can/can’t or should/shouldn’t eat. It’s wild to me that there are countless people in our world who misunderstand that a diabetes diagnosis automatically eliminates certain food groups from an individual’s diet.
Let me say it louder for those in the back who can’t hear: People with diabetes can eat whatever they want. Diabetes varies from person to person, and so do dietary preferences – so just because one person with diabetes might follow a strict keto diet, it doesn’t mean that ALL people with diabetes do. It doesn’t make it right or wrong for a person with diabetes to choose or not choose to eat certain things – period, bottom line, end of the story.
And by the way – I took a big old bolus of insulin for aforementioned pizza and insulin and my blood sugar didn’t spike past 188 mg/dL several hours later – score! So I’m also using this blog post to remind myself that it’s okay to eat “treat” foods like this from time to time, and that does not make me a bad diabetic.
This is a post by Pramita Jasuja that was originally published on the T1International blog on April 9, 2021. I am sharing it here today because I thought it was an interesting take on how type 1 diabetes is (or in this case, is not) recognized in another country. Thank you to Pramita for sharing her story and explaining the importance of legislation in advocating for people with diabetes.
Every new type 1 diabetes (T1D) diagnosis can be intimidating, both for the person and the family members. Many people with T1D are told they should be able to live a “normal” life and that they can do everything that a person without diabetes can do.
As a newly diagnosed child with blood sugar levels of over 570mg/dl, all that was on my mind was T1D. But a year post-diagnosis, when daily needles became the new normal, I was told by my family that I was completely fine and that there “was no need to tell anyone” about my medical condition. “I am normal” was stuck in my mind and I took it very seriously. So much so, when my endocrinologist asked me as the “patient” to sit near her chair, I replied: “I am not a Patient.” Both my parents and the endo smiled.
It’s been 7 years since that incident and I now reflect on my statement, especially over the word “normal”. Calling yourself “disabled” can have negative connotations attached to it. People often refrain from using that word, as if living with a disability is abnormal. Though if we do this, we deny a part of us. When it comes to legalities, the word “disability” is significant. Disability legislation considers people living with disabilities as subjects who possess rights capable of claiming that they have a disability – not those simply given charitable treatment. This was spelled out in the UN Convention on the Rights of People with Disabilities (CRPD), the human rights convention that hit the highest number of signatories.
I live in India. It’s one of the countries that has ratified this convention, but it’s also a country where myths and stigma overtake the real issues. A report by WHO found that in low-income countries where superstitions surrounding diabetes are common, the fatality rate is high. India is no exception. Due to a lack of proper health care facilities and a lack of national registry exclusively for T1Ds, children in the country are facing late diagnosis and even death. Considering the level of poverty in the country, blood test strips and continuous glucose monitors (CGMS) should be subsidized. Unfortunately, that is not the case. People with T1D are rationing them, which makes diabetes management challenging. Plus high blood sugar levels and/or ketones hinder the ability to perform “normal” day to day activities.
Insulin is like water. Someone with T1D can not live without it, but medical insurance in India does not cover it, and not every type of insulin is subsidized. So for those with T1D and financial struggles, there are the worries about the price of life-giving insulin and medical supplies.
After considering these facts, let’s look at the definition of “person with a disability” under the Rights of People with Disabilities Act (RPWD) 2016 that was enacted after India ratified CRPWD: “a person with long term physical, mental, intellectual, or sensory impairment which, in interaction with barriers, hinders his full and effective participation in society equally with others.”
“When it comes to legalities, the word “disability” is significant. Disability legislation considers people living with disabilities as subjects who possess rights capable of claiming that they have a disability – not those simply given charitable treatment.”
The sad part, however, is that T1D is not considered a disability under this Act, even though the current problems faced by people with T1D in India do “hinder (their) full and effective participation in society equally with others”. I’m arguing that you can not tell every T1D to live “normally” when the condition doesn’t always allow for it. The community is suffering silently and legislative action is being denied.
It is through the recognition of injustices and assertion of our rights that we can ensure equal opportunities. T1D advocacy is emerging in India and as a collective we are highlighting these issues. Change is happening. In 2020 in Kerala High Court, a public interest litigation was filed over the issue of including T1D in the list of disabilities and creating a national registry for people with T1D. This step is important. Recognition of T1D as a “disability” would obligate the government to fulfill what is laid down in the Act, for example providing affordable and accessible health care, ensuring the implementation of non-discrimination clauses and creating special faculties at educational institutions.
Seven years after that endo visit incident, even though I will never be able to deny that I am a patient, what I can do is advocate for patient rights. At a macro level this means standing up for the community. Recognition under the legislation of people with diabetes as those with disabilities is the first step, a chapter in the book of advocacy in my country of India.
Across social media, I keep seeing the same type of photo pop in my feeds that sparks jealousy, triumph, fear, confusion, and hope all at once: the COVID-19 vaccine selfie, fondly referred to as the “vaxxie”.
I’m beyond happy that dozens of family members and friends have received the vaccine. It makes me feel good to know that they’re doing their part to help protect themselves and others, and it’s wonderful to know that the vaccine is being distributed to some extent.
However, I take issue with part of the distribution plan in my state.
Using my voice to hopefully change/improve the rollout of the vaccine in MA felt good.
In Massachusetts, COVID-19 vaccine rollout has been chaotic, to put it mildly.
It’s probably similar in many states, but the part that I find most frustrating is the fact that people with type 1 diabetes (and seemingly no other co-morbidity) are being lumped together with the last group of individuals to be vaccinated.
My endocrinologist confirmed this for me the other day during my virtual appointment: “Why is it [presumably her computer system] showing you in phase 3? You should be in phase 2…” I nodded vigorously and we talked for a few minutes about how disconcerting the whole vaccine rollout plan is. I explained to her that the Massachusetts chapter of #insulin4all was coming up with language to email to local representatives to implore them to do everything possible to prioritize vaccination for all people with diabetes, and a couple days later, I got my chance to do just that.
I looked up my local and state representatives with a quick Google search and emailed three individuals who are in positions to revise public guidance regarding COVID vaccinations. As soon as I hit “send”, I felt this amazing sense of empowerment – it felt good to do something about an issue that I’m very passionate about.
While I wish that I could do more to ensure change, I do feel a sense of pride that I tried to do something by using my voice. It represented the first (but certainly not the last) time that I plan on contacting legislators to help improve diabetes care, management, and accessibility of supplies – not just for myself, but for all people living with diabetes.
This post originally appeared on the T1International blog on November 30, 2020, and it was written by Marina Tsaplina. I am sharing it here today because it made me start to think about creativity and activism as a unit for the first time. Want to know exactly what makes it so powerful to join art with activism? Read on…
When I think about activism, I think about creativity. The two are inseparable. Think about how much creativity and strength it has taken the #insulin4all movement to:
Counter the stories put out by the for-profit U.S. health industry about why insulin “has” to be so expensive and transform the national narrative around insulin affordability
Continually transform the pain in our community into stories for change
Imagine a world where insulin is affordable and accessible for every single person who needs it to live.
#insulin4all, as a banner of the movement, is itself an act of fierce creativity. It imagines a world that we do not yet have, one that countless activists are organizing to bring forward. The courage and imagination that this statement holds brings forward a vision for the world we want to see. It makes it possible to strategically identify those whose actions harm or block us from achieving this vision. And under the banner of the #insulin4all vision – this dream that we are turning into a reality – we organize and strategically map out the steps we must take in order to achieve the world we want to see.
#insulin4all also means a different thing for each of us: each person who joins the movement has their own personal meaning and reason for why we join. And it is these deeply-felt personal stories that make adding art into advocacy and activism actions so powerful. It is another way to bring our personal voice into a collective movement for change. It is also fun!
Here are five reasons – showcasing #insuiln4all and other social change movements around the world – why joining art, creativity and activism together is so powerful. It fosters self-expression, community building, activation, it is inspiring and attention grabbing, and it leads activists to better engage with the media.
1. Self Expression
Getting creative helps hone your personal advocacy voice, transforms a personal feeling into a political message, and contributes your creative spirit into collective creativity. It also helps people feel that every single person’s voice matters. Because each voice does matter. Community art making is a deeply democratic process.
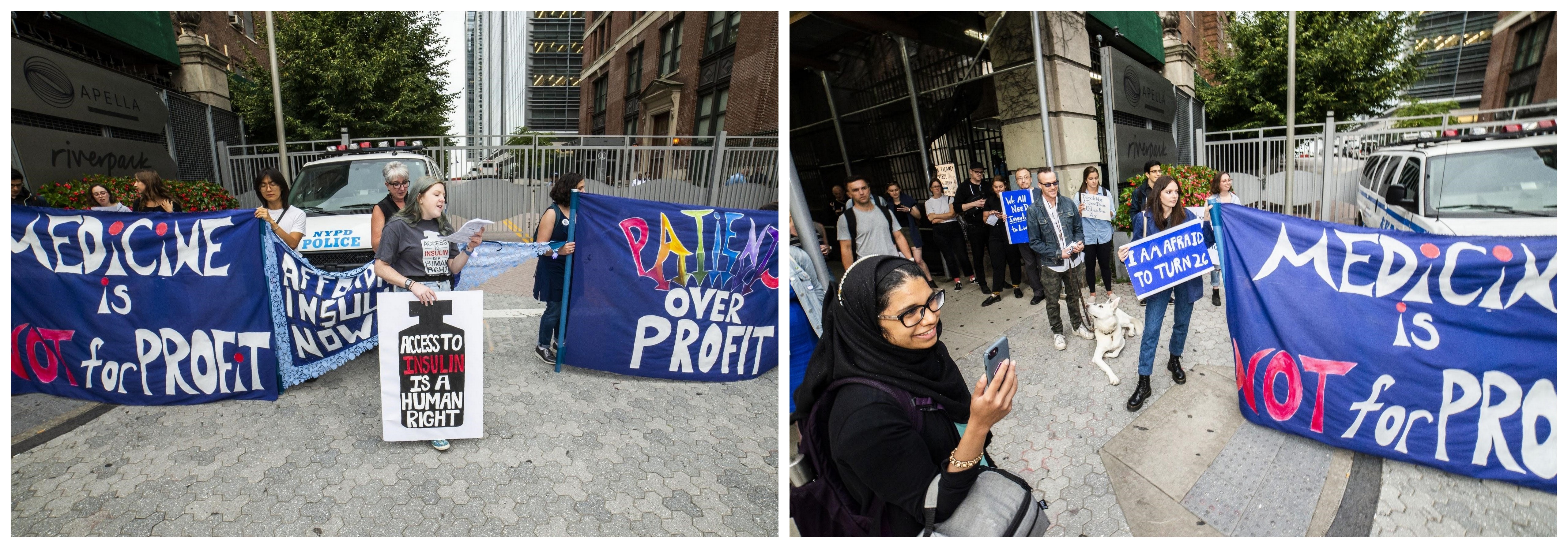
Patient activists pictured below are expressing their personal stories. As another example, signs created by individuals from the disability community NoBody is Disposable call for an end to the discriminatory medical rationing policies during #COVID19.
2. Community Building
Working on an art-build is a fantastic way to build community. Pictured below is one of the in-process photos from advocates making large banners for the New York #insulin4all Chapter and actions. The Chapter was still new and forming, and the art-making process, as well as the many advocacy actions the Chapter continues to do, forms connections between the members. Yes, it takes energy and effort, but once you’ve done it, you have the materials to use in many future actions! Not to mention, people showing up to contribute helps each of us know we are not alone in this fight.
This below pictured postcard was designed by New York #insulin4all Chapter member Annalisa van den Bergh for advocates to fill out and send to the governor. This is a great example of digital (and safe!) advocacy during COVID.
Community artist and organizer Rachel Schragis created screen-printed signs and banners, and led on the creation of many concepts for the Sunrise Movement, because climate health = public health = our health.
3. Political Activation
There’s no one right way to join creativity and advocacy – the image here shows the powerful way an imprint of a red hand across the mouth united indigenous women and allies across Turtle Island (United States and Canada) to bring awareness to the gender-and-race-based violence being perpetrated against indigenous communities.
Being immersed in creative energy opens the space within people to reflect on their own experiences, share and unite in dialogue with others, share opinions, build knowledge and commit to actions. People may often feel embarrassment, or shame, for being unable to afford insulin. This is how oppression works: we internalize external causes and place the blame on ourselves. Creative activism helps activate and engage a person to realize that their suffering has social origins, and helps inspire them to become an advocate and activist who works for policy change.
4. Inspiration and Attention Grabbing
To build energy and grab attention of the public to join your cause, there’s no better way than through creating a bit of a public spectacle. The large banners that the New York Chapter created took up space, and made our messages loud and clear for both the media, and passers-by. The portraits below of the lives lost to insulin rationing by artist Mike Lawson created a deeply-felt homage in helping us mourn the sons, daughters, sisters, brothers, mothers and fathers we have lost to pharmaceutical greed.
Giant puppets have a long and deep history in activism, including the HIV/AIDS movement and beyond. Little Amal, a giant refugee puppet, embarked on an epic journey from Syria to Europe in order to “rewrite the narrative about refugees”.
5. Media Engagement
Finally, by uniting creativity, purpose, emotion and action and creating attention-grabbing visuals, our cause is more likely to catch the attention of social media, and the press. Strong, clear messaging, unique perspectives, and inspiring visuals unite joy, inspiration and purpose in the long, winding road of social change.
Most of all, art and creativity helps us remember the most important thing: We are unstoppable, and another world is possible!
This post was written by Quinn Leighton and it was originally published on the T1International blog on July 8, 2020. June may have been Pride Month, but it’s important every day to understand the challenges faced by the queer and trans communities on a daily basis and raise awareness. Thank you to Quinn for sharing your story, fighting for LGBTQ+ justice, and supporting efforts to make insulin available and affordable for all.
I remember stepping up to the counter to check into an appointment with a new medical provider, when the woman at the desk asked me to step to the person to her right saying to her colleague, “Can you help this…” I had to finish the sentence for her, “person. I’m a person.”
I have often felt fear and uncertainty as a person living with Type 1 Diabetes: when I wake up in the middle of the night confused, reaching for my glucose tablets because my blood sugar reads between 40-50; when my spouse is driving me to the ER because I can’t stop throwing up or get my ketones down while I’m home sick with the flu; and of course the overwhelming financial burden we face daily and monthly in order to stay alive and as healthy as possible.
All of this is assuming we don’t face additional barriers such as discrimination, bias or mistreatment the moment we walk through the front door of a pharmacy, or a provider’s office simply based on who we are and how we show up in the world. For people in the LGBTQ+ community, such as myself, this fear is real and based on lived experience. I am queer, non-binary and married. I’m also white, and acutely aware that while my experiences have filled me with anxiety and have led at times to delaying medical care, I recognize I have not experienced medical racism in the way an LGBTQ+ person of color likely has.
“We must recognize LGBTQ+ people often do not receive the same level of treatment or care that non-LGBTQ+ do, and LGBTQ+ people of color – particularly transgender women of color – are at the highest risk of discrimination, mistreatment and fatal violence.”
Delaying care due to these fears as a queer or trans person is not uncommon in any medical setting, however if you delay care living with diabetes, it can lead to life-threatening complications or even worse. It’s imperative that LGBTQ+ people living with diabetes and other chronic illnesses have the security, affirmation and resources to access the care they need.
We also know that LGBTQ+ people, particularly transgender and non-binary people make less money, despite having the same, if not higher levels of education as their cisgender, heterosexual peers. Even with a patchwork system of employment protections across communities, states and now federally; discrimination in the workplace is still very real. Among LGBTQ+ people, cis-bisexual women and transgender people have particularly high rates of poverty at 29.4%.
Together we can work toward greater health equity, but collectively, we must recognize the disproportionately high impact of poverty, violence, prejudice, mental health issues, discrimination and fear that so many LGBTQ+ people face living with diabetes. We must recognize LGBTQ+ people often do not receive the same level of treatment or care that non-LGBTQ+ do, and LGBTQ+ people of color – particularly transgender women of color – are at the highest risk of discrimination, mistreatment and fatal violence.
Understanding these inequities is paramount in moving forward in advocacy for affordable and accessible insulin for everyone who needs it, particularly those most vulnerable to bias, mistreatment and discrimination. This includes healthcare policies protecting people with pre-existing conditions and protecting LGBTQ+ people from discrimination when accessing healthcare. Efforts to repeal or rollback protections put into place through plans such as the Affordable Care Act that seek to provide care to people who need it most, particularly during a pandemic, is simply cruel and will only result in more harm and negative health outcomes. Non-discrimination protections are critical in providing the care needed for so many LGBTQ+ people living with a pre-existing condition such as diabetes, who already face a gamut of uphill battles in other areas of daily life.
Queer and trans communities are formidable. They overcome extraordinary obstacles to gain economic self-sufficiency, put a roof over their heads, maintain their health in the best of conditions, and simply exist and live in this world. What I’ve really noticed most is the courage and resiliency to navigate these barriers while celebrating community and showing up as our true and whole selves.
I recognize structural and systemic change won’t happen easily or quickly; however, I am hopeful that the movements around us will support communities of color, particularly black and indigenous people fighting for their lives and Asian people under attack due to prejudice and misinformation surrounding the COVID-19 pandemic. I am hopeful people will elevate their support of LGBTQ+ people and those most vulnerable within our community while working to make insulin affordable so that no other person living with diabetes is forced to make life-threatening decisions. And it is my hope that this momentum of support will carry us forward toward justice.
This post was originally published on the T1International website on May 6, 2020, and was written by Rosie Collington. I am sharing it on Hugging the Cactus because to be quite frank, I never understood the many issues surrounding insulin price increases. After reading this post, I had an “aha!” moment as I finally began to understand how the profits from insulin price increases are distributed. It’s an important issue to understand: with increased awareness comes an increased drive to make change.
Patients living with type 1 diabetes have known for years that the list price of insulin in the United States has soared. They’ve paid the price – in insurance premiums, in upfront costs, and also, tragically, in some cases with their health.
But until recently, it has been difficult to prove just how much the list price of insulin has increased, and what proportion of the higher costs for patients have gone to the three main insulin manufacturers – Eli Lilly, Novo Nordisk, and Sanofi – versus other companies in the US prescription drugs supply chain, like insurance companies, pharmacies, and pharmacy benefits managers. Information about pricing negotiations is considered a trade secret, meaning that the actual data is difficult to access. Instead, researchers and patient groups have had to more or less rely on guesswork to estimate the value of price increases, or the highly selective data published by the companies themselves, which do not paint the full picture.
The lobby group representing pharmaceutical companies in the United States, PhRMA, has suggested that pharmacy benefits managers (PBMs) have been the primary beneficiaries of the sharp list price increases of many prescription medicines in recent years. The American Diabetes Association’s Insulin Access and Affordability Working Group similarly reproduced selective data released by the three insulin manufacturers on the differences between the list and net prices – the amount the manufacturer receives – of a few insulin medicines, suggesting that the additional profits accrued by the manufacturers was low relative to intermediaries like PBMs.
This slideshow requires JavaScript.
But in March of this year, researchers at the University of Pittsburgh provided evidence that the net price of insulin medicines in the United States had also soared – by 51% between 2008-2017. This indicates that while other intermediaries had benefited from list price increases, the manufacturers had too. This may seem obvious, but having data to prove it is important.
For my research with Bill Lazonick, funded by the Institute for New Economic Thinking, it has been key to mapping how the profits from higher insulin sales revenues have been distributed. We wanted to find out whether insulin list price increases in the United States had contributed to higher research and development (R&D) investment by the companies, as they so often claim is the case. What we discovered was that as the list price of insulin has increased in the past decade, the ratio of spending on R&D relative to what the companies distributed to shareholders had actually decreased. While over the period of 10 years, the companies spent $131 billion directly on R&D, crucially we found that during the same period, the companies had distributed $122 billion to shareholders in the form of cash dividends and share buybacks.
Cash dividends are the means used by all publicly listed companies to distribute money to shareholders as a reward for holding shares. Share buybacks work quite differently – companies can buy their own shares from the market, which inflates the value of existing shares on the market. Share repurchasing can also benefit company ‘insiders’, like executives, who often receive pay in shares, because they can decide to time when they sell their shares to get the most value. This is not technically illegal, though it was once upon a time. In the last year, some lawmakers in the United States, including Bernie Sanders and Elizabeth Warren, have called for stock buybacks to be banned.
Fundamentally, the system should not have permitted shareholders to profit in this way as diabetes patients were struggling to access their life-saving prescription medicine. As coronavirus continues to spread around the world, the pharmaceutical industry is facing more scrutiny than ever before of its financing and drug development processes. By understanding how value is extracted by shareholders in the pharmaceutical industry, and what relationship this has to patient access, we can, hopefully, create a better system.
This blog post was originally published on the T1International website on April 10, 2020. I am highlighting it here on Hugging the Cactus because 1) I think it sheds a lot of light on the healthcare systems in other countries and 2) it’s a reminder that we’re all in this together.
Hear from ten people living with type 1 diabetes as they share their perspectives about the impact of the coronavirus on their country and their health.
Bolivia – Laura Things are complicated here, and our health system is already problematic. There are no masks and a lack of other correct equipment to treat patients. The government has been very careful about prevention, and quarantine has been going on for several weeks already. Many people are poor and live day by day with what they earn. The government began to give money and food aid to older people and families who receive other types of government bonds, but not everyone can receive it and many say that they do not have enough money to eat. Based on the numbers on our identification, we know when we can go out to get groceries or medications – only on specific days. Still, there is a lot of ignorance and people are not following instructions. There are 200 cases confirmed, with 15 deaths and it is increasing every day. People who have to travel long distances to get medicine do not have good options. I have a friend who has no blood glucose test strips and her blood sugar keeps going too high, but because she does not have test strips, she doesn’t know it. It is very dangerous.
Costa Rica – Dani Our small country is on lockdown, with only 10 people in ICU at the moment. The country is making at-risk patients a priority and currently even shipping their medicines to them to prevent them from going to the hospital and getting infected. Families have been given extra insulin for the next two months, and the community is supporting each other if there is an urgent need for support or extra supplies.
Germany – Katarina Germany has one of the lowest COVID-19 related death rates so far. A lot has been undertaken to prevent the virus from spreading – test centres have opened their doors to the general public, hospitals are increasing their capacities for intensive care and ventilation, and research teams are working hard to improve diagnostics, therapy and find preventative methods. The pandemic is challenging our healthcare system, our economy, and our society, but it also opening new pathways. A lot of diabetes care centres are transitioning to telemedicine, and people with diabetes can get prescriptions and supplies by mail. Being a doctor on the frontline and a high-risk patient at the same time is not easy – I am constantly torn between my profession and my wish to self-isolate and stay safe.
Ghana – Yaa With the rise in COVID 19 cases in Ghana, the government made it mandatory to close down schools for a month, to limit the number of people to no more than 25 in a social gathering, and to start a two week partial lockdown in contiguous districts (3 regions). This means no one is allowed to go out unless it is to buy food and drugs. Borders are closed, and importation of goods are restricted. For people with type 1 diabetes who get supplies at the government hospital using the national health insurance scheme, they still have to go all the way to the hospital for their supplies. The hospital is a major reservoir of the virus, so it increases the chances of people with type 1 who are already at high risk. The only other option is to go buy from the pharmacies, where there is currently a surge in prices. People with diabetes were asked and encouraged to stock up on their diabetes supplies, but not everyone was able to do this. We fear for the unknown and the long term impacts.
India – Apoorva As a medical doctor I have been working and seeing new cases, but now my entire department is in isolation. I took steps back to prevent getting sick. Delhi is one of the hotspots, and we had sudden surge in cases. Rural impoverished areas are problematic due to people living in close quarters. Our government initiated a lockdown, but many tried to leave quickly, especially migrant workers who come and go from the city centres because they lost their livelihoods. This caused the virus to spread despite drastic measures taken by the government. Currently, there are no insulin shortages as all medical services and pharmacies are operational, but we have seen a possibility of analogue shortages and hope to try to ensure that does not happen. Our main aim is to support the actions of the government and I plead everyone to stay home and protect their families.
Enter a caption
Kuwait – Mohammad We have been on lockdown for four weeks, and people who came to Kuwait from other countries were tested. If someone had symptoms, they were put in quarantine. Cases have been contained and so far, there has only been one death. It is interesting that there is now a COVID-19 database that was created rapidly, but there has never been a database of people with type 1 diabetes in Kuwait. Our medications tend to be provided and some are being delivered. Overall, things are OK now, but we are concerned about access to medication and food supply in the long term because most of it is imported.
Lebanon – Cyrine Our country has been facing tricky political problems for the past five months, since we had a revolution in November. The banks have no money, and there is no money from the government. We can only have access to a specific amount of our money per month. We are facing shortages of medical supplies including ventilators and medical protective equipment. The whole country is in an emergency state now and there are military personnel on the streets. As cases continue to rise, people are only allowed to go out at certain times and we can only walk. I have been on self-quarantine for the past few weeks. What worries me most is the people who already struggled to afford their basic insulin and supplies. With 80% or more of the population having lost their jobs, what are those who cannot afford their insulin doing now? I am trying to help those I know about, but there is no government plan for people with type 1 diabetes. People do not have money anymore, so how can they cover their insulin costs?
South Africa – Estelle Testing here is slow. On April 2nd, I heard only 46,000 tests had been done, which is not even 1% of the population. It looks like we have small numbers of diagnosed patients but there is so much unknown. Apparently there is enough stock of medication for up to a year. Medical aid, our version of insurance, said they will cover all treatment related to COVID-19, so that is a relief. A large proportion of individuals might not be taking it seriously enough. The biggest concern is keeping the virus out of the rural areas, which are densely populated. If it spreads there, it could be catastrophic because we do not have enough hospitals.
Tanzania – Johnpeter We only have about twenty cases identified so far. I am currently in Serengeti which means I am far from cities where cases were confirmed and spreading. I am staying put and I had to cancel my doctor appointments and other appointments. I have had to reduce my insulin dose because I cannot get any insulin here in this rural area. I have some insulin in Dar es Salaam that my doctor gave to my brother for me. So right now I am working with my brother to try to find a way to get the insulin. I am not supposed to travel to cities to risk my health, but I am risking my health by staying here without insulin. It is incredibly stressful on top of the challenges I already face accessing and affording my insulin.
USA – Karyn In Georgia, where I live, we are also on lockdown, with cases increasing every day. The biggest issue is shortages of ventilators and protective equipment for hospital staff. Cost and affordability issues are already a problem in the USA and this will likely be an even bigger challenge now. Due to the broken healthcare system here, it’s uncertain if people will even get tested if they go to the doctor. Some people are getting billed for the test even though it has been said they shouldn’t be. Last year around this time, I went to Canada to buy a year’s supply of insulin. I have a bit more, but I’m not sure what I’m going to do without being able to travel abroad this year. I already struggle a lot with the costs. Many people are losing their jobs, and therefore losing their insurance, which will inevitably also impact their ability to afford essential medicines.
As I mentioned in a blog post earlier this month, I’ve sort of known about T1International for a long time now. I knew that they were the organization behind the well-known hashtag #insulin4all, but I was curious to learn more about them and their mission.
As I discovered, T1International works to support local communities by giving them the tools they need to stand up for their rights so that access to insulin and diabetes supplies becomes a reality for all. They have a plethora of materials and information on their website that helps those who are interested become well-versed in this issues surrounding insulin and diabetes supply accessibility. In addition, the T1International team keeps site visitors up-to-date with their blog that contains articles on everything from global stories to legislation explanations.
It wasn’t long before I realized I wanted to work with T1International. So I reached out to their team and applied to become a digital advocate, and less than one week later, I completed my orientation. It’s official: I’m a proud T1International digital advocate.
This is meaningful to me because now I feel more empowered to advocate about the issues that matter, such as the #insulin4all movement. This movement is so important because access to insulin, no matter who you are, where you’re from, or what type of diabetes you have, is critical to the health of all individuals who rely on insulin to live.
Before I dive more into the insulin crisis, let me first acknowledge that I am extraordinarily lucky and privileged: Insulin affordability has never been a personal issue for me. Sure, I’ve had to pay way more out of pocket than I’d like to in order to cover the cost of insulin, but I’ve never had to make the impossible choice between paying for a month’s supply of insulin OR paying for monthly rent.
Many people have had to make that sort of choice, though. And that’s simply not okay.
Whether you’re familiar or unfamiliar with the current insulin crisis, consider the following facts (provided by T1International):
Since the 1990s, the cost of insulin has increased over 1,200%, yet the cost of production for a vial of analog insulin is between $3.69 and $6.16.
Spending by patients with type 1 diabetes on insulin nearly doubled from 2012 to 2016, increasing from $2900 to $5700.
A study of rising drug prices over the decade ending in 2018 found that list prices of insulins increased by 262%, with net prices increasing by 51%.
One of every four patients with type 1 diabetes has had to ration their insulin due to cost. Many have died.
These statistics are more than alarming. They’re downright disgraceful, unjust, and have forced patients to resort to drastic measures to stay alive.
Change needs to happen.
This is why I’m humbled, fired up, outraged, and beyond ready to join the T1International digital advocates team and become one more voice who helps to make the issues regarding insulin access and affordability heard.
This means that I’m rapidly approaching the last few days of my acts of kindness challenge…though I certainly do have some ideas on how to keep the positive vibes going in the near future.
Speaking of, I think that Wednesday’s act of kindness will definitely help me make that happen…
Wednesday, 4/29 – Act of Kindness #24: So this one’s really special to me. For months now, I’ve expressed to many people how I want to become a better diabetes advocate. Sure, I have this blog and it’s one form of raising diabetes awareness, but I want to do more. I started looking into some options on Wednesday and it brought me to the T1International website. I’ve had a vague awareness of T1International and their work for some time now – that website is where I purchased my awesome #Insulin4All sweatshirt – but I wanted to understand what they do to a greater extent.
Turns out, they have a pretty awesome mission: T1International works to support local communities by giving them the tools they need to stand up for their rights so that access to insulin and diabetes supplies becomes a reality for all.
After clicking around their website some more, I found out that they are seeking digital advocates who can help spread the word about their organization and its goals…so I decided to sign up to become a digital advocate for T1International and I couldn’t be more thrilled about it.
I’m learning more about what I will specifically be doing this weekend, but as for now, I’m just excited about the chance to advocate for a cause that I’m very passionate about, which is access to insulin for all. Because like it says on the T1International website, life with diabetes is complicated enough…nobody should have to worry about access to vital insulin, diabetes supplies, or medical care on top of it.
Water and insulin are two very important liquids that not all people have access to…and that’s not okay.
Thursday, 4/30 – Act of Kindness #25: You know what else everyone should have access to, but unfortunately, many people in the world do not? Clean water.
Access to clean drinking water is absolutely something that I take for granted…and it’s simply unfathomable to me that 785 million people – which is to say, 1 in 9 – lack access to safe water. How wild is that? Water is crucial to so many aspects of life, and there isn’t one single human on this planet that can survive without it.
So after a conversation with my mom yesterday about causes that are near and dear to our hearts, in which she reminded me that for years now she’s been hoping to build a water well in a place that it’s greatly needed, I donated to water.org. Talking with my mom and hearing the dedication in her voice made me want to do what I could to help her support a cause that means a lot to her, so I happily made the donation in her name and even got to send her an eCard notifying her of it. Hopefully, it makes her smile and reminds her that she does have the ability to get that well built one day because those closest to her will support her every step of the way.
Whether it’s insulin, water, food, shelter…there are simple basic needs that all human beings deserve to have access to, and its an injustice that they don’t. Fortunately, there are amazing organizations out there like T1International and Water.org that work tirelessly to change this, and it’s humbling to be able to support them in any capacity. I linked to their websites in this post – hover over their names above – I encourage you to check them out and consider the ways you might be able to help them, too.
It’s November 6th which means that it’s Day 6 of the Happy Diabetic Challenge! Today’s prompt asks us to name our diabetes hero/heroine. Well, I have more than one…
My diabetes hero is not just one person. It’s a small group of people that I call my family. (Awwwww, how sweet.)
Me with my heroic diabetes family.
My mom, dad, and brother are all-too familiar with diabetes. My mom is T1D, like me, and my dad and my brother were the lucky ducks who got to live under the same roof as us for many years. All three of them are diabetes heroes to me, but in some very different ways.
Let’s start with my brother. He is three years older than me and I’d say we were fairly close to one another in our shared childhood. Though he doesn’t share a diabetes diagnosis with me, he grew up with diabetes just as much as I did. And do you know what’s amazing about that? I’ve never once heard him complain about it. If he has ever felt any fear or worry for my mom and I, he definitely has done a good job of internalizing it. He treats us like we have normal, functioning pancreases, and I think the reason for that is he knows that we are more than capable of taking care of our diabetes ourselves. Although his thoughts and feelings about our diabetes have yet to be verbalized, I appreciate his unique brand of support for us and I continue to be wowed that he never seemed to be bothered by the extra attention I got as a child due to my diabetes. No unhealthy sibling rivalry there!
Next up is the other Type None in our family: my dad. I’ve written about my dad in a couple of previous blog posts. He is truly the Mr. Fix It in our family. If there is a problem, he wants to solve it – especially if it is something that is causing his loved ones emotional distress. He has had more than his fair share of situations in which my mom or I were seriously struggling with our diabetes. I can only imagine how he feels when all he can do is just stand by and let us work through our issues: It’s probably a combination of helpless, angry, and worried. He’s said numerous times over the years that he’d give my mom and I his healthy pancreas if he could, and I’ve never questioned the sincerity behind that sentiment. I know he means it, and to me, that’s the kind of heroism that nobody else in my life can even begin to compete with.
And then we’ve got my diabetes partner-in-crime, my mom. How on earth she managed to deal with her OWN diabetes, in addition to mine, all throughout my childhood is completely beyond me. Besides being there for me as a source of unwavering emotional support as someone who really “gets it”, my mom’s attended practically every single endocrinology appointment with me, encouraged me to start using an insulin pump, ordered alllllll of my supplies for many years (and kept track of the stacks of associated paperwork), and helped keep me as calm as humanly possible throughout my terrifying insurance transition that took place late this past spring. Let me just restate that she did all of this and still does all of this while still dealing with her own diabetes!!!!! It’s sort of mind-blowing to me that she can stay so much calmer about her diabetes than I ever could when it comes to either of ours, but she does it, and that makes her a heck of a diabetes hero to me.
What’s really neat about my diabetes heroes, as a collective unit, is that diabetes has never and will never define our family. It’s something that lingers there in the background, for sure, but it almost never steals our attention away from our time spent together. I can’t recall a single instance in the last 22 years that diabetes really, truly disrupted our family rhythm (maybe my parents would disagree with that and count in my diabetes diagnosis, but I barely remember that).
It just goes to show that even as something as life-altering and disruptive as diabetes only made my family stronger when it hit us with a double dose.