A few years ago, I wrote a blog post about how I received a shattered insulin vial in my mail order pharmacy delivery. At that point in time when it initially happened, I’d never experienced anything like that before and was immediately panic-stricken about how I could get a replacement for something that wasn’t my fault, as the vial was smashed upon arrival.
Fortunately, a quick phone call resolved the situation, and I’ve been lucky enough to receive fully intact insulin vials in the mail every 90 days or so ever since. But imagine my fear and concern when I got my most recent insulin delivery and discovered, upon opening the package, that one of my insulin vial’s cartons was totally squished!
The smooshed packaging, in question.
I have no idea how it happened to just one out of the five in the order, seeing as they were all put into the package with the exact same level of cushion and protection. The 5 vials were in a zip-top plastic bag, which lay on top of 3 ice packs, which were surrounded by layers of soft foam packing material, all of which was placed in a mid-size cardboard box. It’s not like the squished insulin carton was separate from the other four in any fashion, so truly, I’m at a loss as to how it got so severely misshapen. But what I can say is that I was beyond relieved when, after further inspection, I found that the vial was fully intact – not a drop of insulin missing from it nor a crack in the glass to be found. Phew! Momentary worry faded into reassurance that I wouldn’t have to make any phone calls to obtain a replacement, and that all I had left to do was put my new insulin vials in the butter compartment of my fridge (naturally) with my remaining old vials.
Squished upon arrival, but definitely not destroyed – though a good reminder nevertheless to always inspect my insulin when it’s delivered, just in case any surprises await me.
Just over a week ago, Eli Lilly announced a 70% reduction in price for its most commonly prescribed insulins that resulted in a cap of patient out-of-pocket costs at $35 or less per month.
This news was huge and spread like wildfire across the diabetes online community. And for good reason – it’s something that so many people with diabetes have needed to happen for a very long time. Most reactions I saw were that of complete and utter joy and relief. I’ll admit that’s what I felt at first, too, until I saw the more displeased responses that directed additional frustration and rage at Eli Lilly for not taking this action sooner, or reducing the cost of insulin to make it free altogether. Those posts got me thinking.
I’ve had time to reflect and gather my thoughts on the matter, and I think I land somewhere between thrilled and bummed, myself.
This news is absolutely something to be celebrated, as it will undoubtedly assist people who struggle to afford insulin with astronomically high price tags. This is an issue that I’ve spoken about on the blog before, and while I feel very fortunate to never have personally struggled with affording my own insulin (though I’ve certainly complained about out-of-pocket costs in the past), I’ve read countless stories about individuals in the United States who’ve had to take drastic measures in order to obtain this life-saving medication. So this news is wonderful, for sure, but it also feels a little too late.
Is this response from Lilly induced by the pressure that they’ve felt from diabetes advocates in the last several years? Is it a genuine call to action to other insulin manufacturers to follow suit and slash prices? Is it all just some sort of PR stunt? My suspicion is that it’s a mixture of all three, and while this feels like a victory for now, I don’t think that I will personally be satisfied until all people with diabetes are able to get insulin for free – no bottom line, no gimmicks, no nothing other than access for all.
Valentine’s Day is tomorrow. Whether you love or loathe the day, it’s an occasion that’s synonymous with chocolate, love, and flowers; more specifically, a dozen red roses.
A dozen red roses is a classic Valentine’s gift. But what if you received 11 roses in your bouquet, instead of 12? What if you knew that a rose was spared because the value of that flower helped provide insulin to someone who needs it to live?
I bet you wouldn’t mind getting one less rose in that case. And it might just make you like the holiday a little bit more!
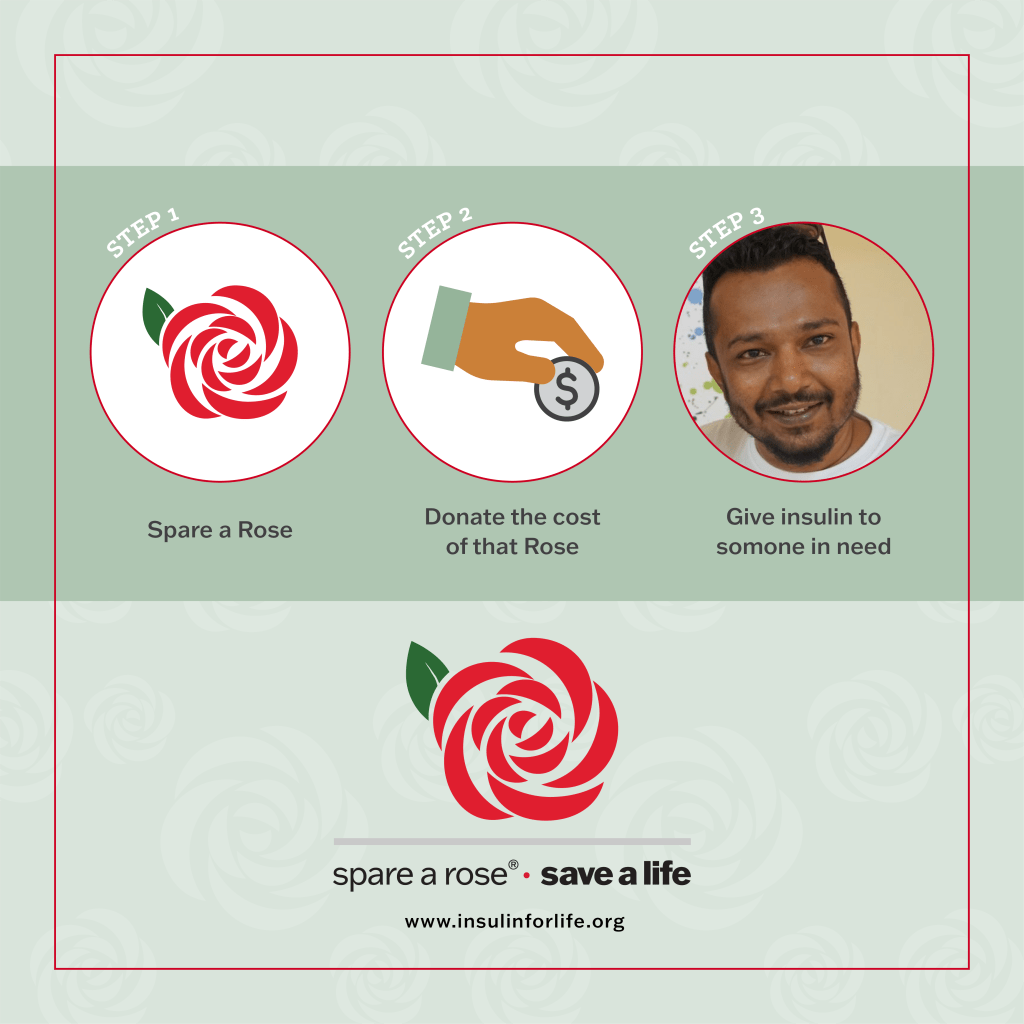
A little bit of history: Nearly 10 years ago, folks from the Diabetes Online Community (DOC) started the Spare a Rose campaign for the organization Life for a Child. This campaign was able to give insulin and diabetes supplies to children and young adults with T1D in under-resourced countries. Last year, these individuals looked at how they might be able to support all people with diabetes, seeing as the need for insulin and related supplies and care lasts well beyond childhood.
Thus, Spare a Rose, Save a Life was born! Donations to this campaign go to Insulin for Life, a charity that provides resources, education, and advocacy to many of the same under-resourced countries that were supported by the original Spare a Rose campaign.
It’s an absolutely wonderful idea that will positively impact – and save the lives of – even more people living with diabetes who need access to vital medication, supplies, and healthcare.
I’ve written about the Spare a Rose campaign here on Hugging the Cactus for years now because it’s a beautiful way to celebrate a day that makes some swoon and others sick to their stomachs. A common complaint among people in this day and age is that too many holidays are all about raking in the dough for companies like Hallmark; in other words, most holidays have lost their original meaning and have become too commercialized.
So here’s your chance to bring back some significance to Valentine’s Day. In the light of the health challenges the world has collectively faced in the last couple of years, it’s more important than ever that we do all that we can to help people with diabetes access life-saving supplies and care.
Learn more about Insulin for Life, Spare a Rose, and donate here.
If there was a rulebook devoted to the do’s and don’ts of life with diabetes…it would be quite the tome. I imagine it to be as long as the fifth Harry Potter book, which had 766 pages and weighed just shy of 3 pounds, though it would certainly not be as engaging of a read.
As I started to visualize a diabetes rulebook, I started thinking about the actual rules it would list out. It would cover the basics, for sure, of life with diabetes, like “count carbs at every meal” and “remember to take your insulin”. But it would also get into the minutia – the things that aren’t so obvious, even to those who are fairly well-versed in diabetes. Things that I didn’t know until adulthood, like how glycemic index, alcohol, caffeine, dawn phenomenon, and so much more can affect blood sugar levels.
Yeah, it would definitely be a boring-ass read.
The diabetes rulebook would probably resemble this and look completely, utter unremarkable (otherwise known as BORING).
But as I was coming up with a seemingly endless mental list of diabetes rules, it stuck out to me that there’s one that I don’t follow. In fact, I’m not sure that I ever followed it. And that rule pertains to insulin.
The rule is about how if you open a vial of insulin, it’s best to use it within a 30-day (or maybe it’s 28-day) window. I think it’s because manufacturers claim it loses its potency after that timeframe passes, but to me, it’s a bunch of BS.
Maybe I do go through whole vials of insulin in a one-month period, or maybe I don’t. I have no clue, I don’t keep track of my supplies to that extent. But what I do know is that “expiration dates” and “best by” labels aren’t always based on exact science. I’ve totally eaten my fair share of “expired” foods (things like granola bars or cans of soup, definitely not wilted spinach leaves or moldy yogurt) because I use my common sense when making judgment calls about consuming those items. For me, it works kind of the same way with insulin. As long as an insulin vial has been properly stored since opening it (in a refrigerator’s butter compartment, because of course), then I feel safe using it beyond a 30-day period – again, within reason, using logic (I doubt that I’d use insulin dated YEARS ago).
I’ve even heard of folks using insulin that’s past it’s expiry date, and while I haven’t done that myself, I can’t say I blame anyone for trying to use up every last drop of the stuff when it’s in possession and it’s necessary to take. It’s too expensive to waste.
So if by breaking this “rule” makes me or other people rebels, I’ll don the title with pride…and smirk to myself as I think about other diabetes rules (ahem, pertaining to prolonging CGM sensor life, or using sites other than the abdomen for my Dexcom, or hardly ever remembering to change my lancets…) that I’ve broken over the years.
This post was originally published on Hugging the Cactus on December 16, 2020. I’m sharing it again today because this was a fun and festive (if not messy) craft that I did with an insulin vial that I saved. Currently, I have about a dozen or so empty insulin vials set aside and I’m wondering what kind of craft I should do next…
I love Christmas, crafting, and some might argue that I love T1D (that’s mostly false, but when you’ve got a chronic illness, you’ve got to learn how to love some aspects of it…otherwise, you’ll be miserable).
So I recently *attempted* to combine all three of these things and do a little DIY project with an empty insulin vial.
And I learned a few things along the way…
I do not recommend messing with a glass vial without safety glasses, gloves, and a trash can nearby. I was lucky enough to avoid any major glass breakage, but some did happen, and I could totally see this craft getting wicked messy and potentially ouchie without taking the proper precautions.
Insulin vials are stable AF…they are not meant to be tampered with.
Glitter cannot be directly injected into an insulin vial. Period, bottom line, don’t even try it.
Okay, so now that I’ve got my disclaimers/lessons learned out of the way, let me tell you why I decided to fill an empty insulin vial with gold glitter.
For years, I’ve seen DIY projects floating around online involving old diabetes supplies. They range in the level commitment and skill involved, but there’s no questioning the creativity of our community when it comes to recycling supplies we’d normally throw away after using.
One project that I’ve seen over and over again is transforming an empty insulin vial into a Christmas ornament: Simply stick an ornament hook into the insulin vial’s rubber top, hang it on a Christmas tree branch, and bask in its beauty. I decided to take this concept to the next level by putting gold glitter into the vial because insulin is often referred to as “liquid gold” within the diabetes online community. What better way to represent that than to make it appear as though the contents of a vial were truly liquid gold?
In order to do this, I set aside a vial once I was finished with it/sucked every last drop of insulin out of it. Then, I made a sad attempt at combining glitter with water and using an old syringe to transfer it to the vial (needless to say, I had no luck). So I came up with a new strategy: Pierce the rubber stopper and try to funnel glitter in…and that didn’t work. It became evident that I’d have to remove the top entirely, so using my nifty new toolkit that my father just purchased for me (thanks, dad), I set about the task. I used a razor to carve the rubber stopper up and out, and then pliers to get the metal maroon covering off completely. I broke off a small piece of glass in the process – whoops – but using those tools did the trick for me…all I did after that was take the cap from a new vial of insulin and glued it to the top of the glitter vial to ensure most of its sparkly contents would remain inside.
And voila, here’s the end result:
Despite the glass breaking off, this DIY came out better than I expected.
As I held the glittery vial in front of my Christmas tree for a few photos (if I didn’t take pictures, then it didn’t happen), it occurred to me that there’s a strong likelihood that many families will have to make a difficult choice this holiday season: Give a special gift to a loved one, or use that money to pay for insulin instead. Or even more seriously, to have to choose between making this month’s mortgage/utilities payments, or getting life-saving medication.
The thought shook me, as nobody should have to make a choice like that ever.
And so I thought of something to add to my Christmas wish list: affordable insulin for all.
This post originally appeared on Hugging the Cactus on September 23, 2020. Just over one year later, I’m sharing it again because it’s a reminder that life with diabetes is filled with the unexpected, and it’s important to be proactive when dealing with these curveballs. Read on to find out how I handled the broken insulin vial…
As soon as I opened the package, I knew something was wrong.
The contents of said package were five vials of insulin – my regular 90-day supply. On the surface, nothing seemed wrong. They arrived in their usual styrofoam cooler that was taped shut. After removing the tape, I saw four ice packs next to the plastic packaging containing the insulin vials; again, this was all expected.
When I picked up the plastic package and used scissors to cut it open, though, a pungent odor greeted my nose.
A medicinal, harsh, familiar scent…the smell of insulin.
Upon further investigation, I discovered that one of the five cardboard boxes encasing the vials was totally damp to the touch. Gingerly, I opened it from the bottom flap, which was sticking out slightly due to the wetness. That’s when I saw the shattered insulin vial: Somehow, the bottom part of the vial had broken, spilling and wasting all of its contents.
I wish that smell-o-vision was a thing, because OMG…the smell coming from this was STRONG.
I was shocked. In all my years of diabetes, nothing like this had ever happened to me before!
I didn’t really give my next step a second thought: Immediately, I jumped on the phone with Express Scripts, which is the mail order pharmacy that I use for my insulin and some other medications. I spoke with and explained the issue to a customer service representative, who connected me with a technician that promised a replacement vial would be mailed to me at no additional cost to make up for the broken one. I asked if they needed me to send the broken one back to them, but I was reassured that it wouldn’t be necessary because I had called them so they could document the incident.
My issue was resolved, just like that, in fewer than 15 minutes. While it was annoying to have to take time out of my day to figure that out, I’m very happy that I got a replacement quickly and easily. But really, where was quality control on this one?!
Insulin is expensive, as we all know. And to see that a perfectly good vial full of it was rendered useless due to defective packaging was a major punch to the gut, indeed.
I attended a Massachusetts #insulin4all meeting recently that got me thinking about how good people with diabetes tend to be at minimizing.
I speak for myself, and some other people with diabetes I know, when I say that we’re really good at making it seem like it’s not a big deal. We manage a 24/7, 365 chronic condition like it’s not the full-time job that it is. I have family and friends who occasionally pick up on this and marvel at my ability to be present in a myriad of social situations while discreetly watching my blood sugar levels or calculating insulin dosages. I rarely act like diabetes is as serious as it is and that’s because I’ve become an expert at making it seem like small potatoes in my life.
And I’m not just good at minimizing my diabetes – I’m also highly proficient in minimizing the fact that it has forced me to make difficult decisions in my life, particularly when it comes to financial choices.
Over the years, I’ve become excellent at downplaying the impact of diabetes on many aspects of my life.
During this #insulin4all meeting, I was conversing with other chapter members about whether or not we, as individuals, have struggled to afford insulin. And a lot of us confessed that we’ve been pretty lucky and have never really had to resort to making truly difficult choices when it comes to affording insulin or other diabetes supplies. Despite that, we feel passionately about those who struggle to gain access because we understand how high the stakes are – it’s literally a matter of life or death.
But just because we’re able to (for the most part) afford insulin, that doesn’t mean that we haven’t had to make certain choices that we might not have had to make if we didn’t have diabetes.
For example, when it comes to my career, I’d never consider a job that doesn’t offer solid health insurance plans. Even if my strongest desire was to be a freelance writer, I wouldn’t go through with it because I know that it would be challenging to figure out my health insurance. And I know that the minute I run out of FSA dollars each year, I start thinking about setting money aside just to cover the costs of my diabetes supplies…which means that instead of buying some new clothes or planning a weekend getaway, I sometimes have to sacrifice those luxuries in favor of ensuring I have enough money to cover my fixed expenses as well as my diabetes medications.
When I think about it, of course I realize that it’s not fair, but haven’t really considered it before because this is just how it is. I’m used to it. And so are many other members of my #insulin4all chapter. We’re all accustomed to having to make certain choices about our lifestyles or spending habits that minimize the larger issue of insulin affordability. We’re used to it, even accepting of it, but that doesn’t make it right and it certainly underscores the terrifying fact that too many people simply can’t afford insulin and have to make much tougher decisions in order to get it.
It’s time to become a little less good about minimizing and better at vocalizing – not just the seriousness of diabetes, but also the dire nature of insulin affordability and access that affects millions around the world.
This blog post was originally published on Hugging the Cactus on May 13, 2020. I’m sharing it again today because I think it’s super important to weigh the answers to these questions before deciding to try new diabetes technology. This is coming from someone who waited 17 years before she tried her first insulin pump, and even though it has had an enormously positive influence on my life and sometimes I wish I’d tried it sooner, I’m ultimately glad that I waited that long! Read on for more details…
So you want to try your first continuous glucose monitor. Or maybe you’re ready to leave behind multiple daily injections and switch to insulin pump therapy. Whichever diabetes device you’re looking to start using, there are some questions you’ll probably want to have answers to before decide that now’s the time to introduce new diabetes technology into your daily routine.
The following is a compilation of the questions that I thought long and hard about (literally for years) and that I wish I’d thought long and hard about before I made the transition to the OmniPod insulin pump.
1.Am I ready for it? It took me 17 years before I decided that I was ready to try an insulin pump. 17 freakin’ years!!! I spent most of that time being too afraid of introducing such a drastic change to a routine I’d had down pat for such a long period of my life. There are times when I wish I’d gone onto my insulin pump sooner, but ultimately, I’m glad that I wasn’t swayed by my family or doctors to go on it before I truly felt ready. By the time I started using my OmniPod, I had the maturity, responsibility, and emotional intelligence that I felt that I needed for an insulin pump.
2. Will I be able to afford it? Obviously, this isn’t a question that I wondered about when I was younger, but it’s one of the first things that comes to mind as an adult on her own health care plan. We all know that diabetes supplies are expensive, and it seems that the more technologically advanced something is, the more money that has to be forked over in order to obtain it. This isn’t right or fair, but it’s a simple truth and an important one to think about before choosing one pump or continuous glucose monitor over another.
3.Why do I want to start using it? I wanted to start using my OmniPod because my mom experienced great success when she started using it. And I decided to get a Dexcom CGM because I fell in love with the technology after undergoing a trial period with my endocrinologist. In both situations, I felt very much in control of my decision to start using these devices and I didn’t really listen to anyone else’s opinions. But I am very aware of the fact that social media and real-life friendships with other people with diabetes can often sway people in different directions. After all, if I saw a post on Instagram from a dia-influencer who was singing the praises of a Tandem T:slim pump, then I might seriously start thinking about switching to it (this has actually happened to me). But the bottom line is to think about the why – will this device enhance quality of life for me? Will diabetes be easier to manage with it? Will it help me achieve my A1c and/or blood sugar goals? Do I need to add something new to my routine because I’m feeling burnt out by doing things the same way all the time? Knowing why I wanted to use an OmniPod or a Dexcom CGM made me feel that much better during the whole process of learning how to use them – I felt like I had clear goals that would help me navigate the integration of these new technologies into my daily routine.
Did you know that Insulet/OmniPod has demo pods that you can wear? They don’t hold insulin or deploy a cannula, but they can give you a good sense of what it’s like to wear a pod on a daily basis!
4. Will I be comfortable wearing it 24/7? This is a big one! Pods, pumps, and CGMs are very visible, and it can be jarring to go from being “naked” to having bumps and lumps underneath clothes that can get caught on doorknobs, chairs, and the like. Personally, the benefits of my OmniPod and Dexcom outweigh something like this which is a bit superficial, but that doesn’t mean it’s not something to think about. But it’s also worth thinking about comfort and what is least painful when it comes to insulin delivery, so that’s why this is an important question to ask.
5.Do I know anyone else using it who can provide feedback from a patient’s perspective? I’ve talked about this before, but I’m not sure when, if ever, I would have seriously considered using the OmniPod if my mother hadn’t tried it first. The fact that we both have diabetes has probably made us a little closer and strengthened our bond, so if there’s anyone’s opinion that I’m going to trust when it comes to something like this, then it’s hers. I can actually remember her first few weeks on the OmniPod – in which she learned a lot of valuable lessons – and how pleased she was with it once a few months with it elapsed. She taught me the ins and outs of the OmniPod when I started to use it, and I’d argue that her advice was more helpful than that of my diabetes educator. So I’d advocate gathering opinions from family and friends (if either is applicable) or the diabetes online community before going on a new diabetes device, in addition to the research component below…
6.Have I done enough research on it? …Like any smart shopper, it’s crucial to really consider all options and research them thoroughly, especially when it comes to the top contender. I definitely did not complete sufficient research before going onto the OmniPod or Dexcom; rather, I trusted that they were just right for me. If I were to switch to something else tomorrow, though, you can bet that’d I’d spend a lot of time scouring the web for every last bit of information on the device so I could make the most informed decision possible.
New diabetes technology can be both scary and exciting. But more than anything else, it can really make life with diabetes much more carefree, and I’m glad that in this day and age there are so many options available to people with diabetes that continue to be technologically impressive
The following is a post that was featured on the T1International blog on May 17, 2021. I’m sharing it here today because I want to help spread the word about the Gift to Greed campaign. Learn more about it by reading on (and visiting the links at the end of this piece)…
On Monday, May 17th – 100 years after Banting, Best and Macleod begin their first experiment trying to extract insulin in Toronto – T1International and its advocates around the world launch their year-long campaign. 100 Years: From Gift to Greed will tell the story of insulin’s discovery and how it went from being a gift to the world to a profit machine for the pharmaceutical industry. The campaign will be led by a combination of social media education and a variety of actions.
“A gift to the world has become a tool for price gouging patients all over the world.” – Elizabeth Pfiester, Founder and Executive Director of T1International
Insulin is as essential as oxygen for all patients with type 1 diabetes and many with type 2 or other forms of insulin-dependent diabetes. Globally, insulin rationing is common, and half of those in need of insulin cannot afford or access it. For every two people alive with type 1 diabetes, there is a third who did not survive. The production and distribution of insulin is dominated by three companies – Eli Lilly, Novo Nordisk, and Sanofi – who control more than 90% of the global market.
In the early 1920s in Toronto, Canadian physician and scientist Frederick Banting began working on an idea in the laboratories of J.R.R. McLeod to isolate and extract insulin. Medical student Charles Best and chemist James Collip worked with Banting to test, purify and refine insulin for clinical trials in humans.
After vowing that insulin would not be something to profit on, the discoverers sold their patent for $1 CAD each and eventually passed the rights to the pharmaceutical company Eli Lilly and Co. so that it could be mass produced and widely available. Banting famously said, ‘’Insulin does not belong to me, it belongs to the world.’’
While this incredible advancement was intended as a gift from the discoverers, Eli Lilly and the two other major insulin producers, Sanofi and Novo Nordisk, have turned insulin into profit machines, assisting in bringing in billions of dollars in profit every year. By 1923, insulin was the highest-selling product in Eli Lilly’s history, and profits from it accounted for over half of the company’s revenue. As we know, the prices have continued to skyrocket ever since. Since 1996, the list price of insulin has increased by over 1200% in the United States. Eli Lilly’s Humalog insulin increased in price by 585% between 2001 and 2015 alone.
T1International’s Founder and Executive Director, Elizabeth Pfiester, said, ‘‘A gift to the world has become a tool for price gouging patients all over the world. The greed of the pharmaceutical industry is keeping insulin out of the hands of millions. This greed leads to the loss of countless lives and dampens the dream of Banting and his colleagues, which was to make insulin a gift to the world. It is outrageous that this is the reality, and T1International will continue to speak out until the pharmaceutical industry is held accountable.’’
T1International advocates will be speaking out and educating the community about the story of insulin and how to get involved in T1International and the global #insulin4all movement. The aim is to put an end to the reality that far too many people die or suffer grave physical, mental, and emotional health consequences due to pharmaceutical greed.
This article was written by Elana Megerian and it was originally published on March 24, 2021 on the T1International blog. I’m re-posting it here today because, quite frankly, I found it disturbing. I had no idea that safely navigating encounters with law enforcement was a problem for the diabetes community. I can also admit that I made assumptions based on the headline of this article, but decided to stick with it only to discover that my assumptions were wrong and that the criminalization of diabetes symptoms is a real issue. If you have any doubts about this article, I encourage you to read the full piece so you can understand what’s going on and the steps that should be taken to address it.
When widespread Black Lives Matter protests erupted in the summer of 2020, the diabetes online community began crowdsourcing ideas about how to safely participate. Concerns grew in response to an incident in which police confiscated the supply bag of a protestor with type 1 diabetes, despite her consenting to a search and communicating her need for glucose.
A viral video of the encounter revealed another pressing need of the diabetes community: how to safely navigate encounters with law enforcement. This led me down a rabbit hole that heightened my alarm as I found story after story of police and prisons withholding insulin.
In 2013, footage from Rikers showed Carlos Mercado repeatedly vomiting, fainting, and displaying signs of severe illness in the presence of corrections officers. At age 45, he died after having his insulin withheld for 15 hours.
In 2014, William Joel Dixon was found dead in his cell after his insulin was withheld for seven days. Records show that his blood sugar was only checked once during that week. He was 28 years old.
In 2015, Michael Robinson died after being put in solitary confinement in response to his pleas for insulin. He was 33.
In 2016, Morgan Angerbauer’s death in an Arkansas jail cell was caught on video. Records show that she had been calling out for help, but was ignored. She received no insulin for 23 hours, and her requests for blood glucose checks had been denied. She was only 20 years old.
In all these situations, staff were aware that the victims required insulin to live. In all the cases, insulin was withheld long enough to induce diabetic ketoacidosis, a potentially fatal complication that usually occurs in people with type 1 diabetes who do not have regular access to insulin. It is a torturous and almostly completely preventable cause of death, yet it is far too common in US prisons. Since 2008, at least 12 such deaths related to withholding insulin have occurred in the state of Georgia alone.
“#insulin4all is more than a hashtag: It is a rallying call to everyone impacted by insulin inaccessibility, and a mournful cry for all who have lost their lives while insulin remains clearly in view, but cruelly out of reach.”
Diabetes symptoms have also often been criminalized. In August 2020, Max Johnson, a black man with type 1 diabetes who was having a seizure due to hypoglycemia, was dosed with ketamine by police and Emergency Medical Services (EMS) after his girlfriend called them for help. The same drug that killed Elijah McClain, ketamine was reportedly delivered to Johnson at such a high dose that it rendered him unable to breathe and led to a two-day stay in the ICU. The American Diabetes Association has documented many other cases in which people were denied insulin, or had their diabetes symptoms treated like criminal behavior by police.
These instances flagrantly defy the 8th and 14th amendments of the United States, which protect the right to adequate medical care for incarcerated people as well as those in police custody. Since the law is unequivocal, it is distressing that violations are commonly committed by the very individuals and systems meant to enforce it.
One factor perpetuating this is the lack of recourse for victims and their families. It’s hard to successfully bring a case against the police or a prison. Even if such a case is won, it doesn’t bring back a lost life, reverse damage from chronic hyperglycemia, or ease the trauma of being brutalized by those called in to help you through a medical crisis.
So what can be done? Standards of ethical behavior need to be raised for police, EMS, and corrections officers. Given how common the condition is among incarcerated individuals, anyone working with this population should be educated about diabetes, its basic management, and the signs of acute crisis. Deaths due to subpar medical care aren’t rare occurrences. Chronic illnesses are the leading cause of death in US prisons and are probably frequently covered up.
This disproportionately impacts Black Americans, who have higher rates of incarceration, diabetes, and diabetes-related complications compared to their white counterparts. Diabetes is too often a death sentence in the prison setting. Advocacy for prison reform is urgent.
It is time to recognize that incarcerated people with diabetes are particularly vulnerable to insulin insecurity. #insulin4all is more than a hashtag: It is a rallying call to everyone impacted by insulin inaccessibility, and a mournful cry for all who have lost their lives while insulin remains clearly in view, but cruelly out of reach. It’s a demand for justice for everyone who needs insulin to survive, including incarcerated people with diabetes. We must find ways to meaningfully include and involve this population in our activism.