There IS a definitive best time to change a CGM and/or insulin pump site. It’s rare, but when the stars align and both sites need to be changed around the same time on the same day, then that is the magical occasion that allows for a device-free shower. So for me, syncing up pod and Dexcom sensor changes with the time that I plan to take a shower is by far the most wonderful and ideal time to go out with the old, in with the new.
Think about it. These two devices are meant to be worn 24/7, 365. The only time they ever come off my body is so I can rotate sites and put fresh sensors/pods on. This means that I’ve got two medical devices attached to my body at (just about) all times. And I’m totally used to that, except for the times that I somehow forget about my pod and CGM and manage to knock them off my body while changing clothes or, you know, just walking around – and apparently into – doorways/gates/etc.
So when a pod change coincides with a CGM sensor change, I embrace this as an opportunity to enjoy being free from my devices for a short window of time – and for me, the length of time it takes for me to shower is just perfect for taking a break and not having to worry about 1) cleaning around my devices, 2) bumping them into my shower door, or most importantly of all 3) rising blood sugar levels as this short time span isn’t long enough for me to face any consequences of not having an active bolus.
These might seem like trivial reasons to relish a device break so much, but it really is the only time that I am reminded that my body is aided by the devices, not defined by them. It’s nice to see my skin free of them both, even if it’s only for a short while.
This blog post was originally published on Hugging the Cactus on June 19, 2020. I’m sharing it again today because truth be told, I needed to hype myself up a bit about having my diabetes devices be a lot more visible during the summer months. As I’ve gotten older I’ve grown less comfortable having them on display, but it’s inevitable when I’m wearing short sleeves, shorts, or a bathing suit. Read on to learn about the other things that make diabetes a little less invisible in the summertime…
Sun’s out, guns pumps out, amirite guys?
The summertime season is in full swing, and now that it’s here I’m thinking of the various ways my diabetes is more pronounced in the warmer weather. It’s much more visible, leading to many more questions, but what are the cues that give it away to others? I thought of four…
Visible sites. Shorts-and-t-shirts weather makes it much harder to place pods or CGM sensors in discrete locations. And if I’m going to the beach? There’s no way that I can even attempt to hide my devices. That’s probably why I make them even more obvious with…
…Pump and sensor art. I’ve written about Pump Peelz and GrifGrips in the past – they make adhesives and skins that are specially designed to fit pods, PDMs, pumps, meters, and more. The products they make are truly little works of art for diabetes devices, and I like to make sure all of mine are decked out in the summer months so I can show off tech that’s not only functional, but also stylish.I’m looking forward to donning my best beach-y Pump Peelz on what I hope will be many trips to the beach this summer.
It’s tough to “hide” diabetes in the summer when short sleeves and tank tops become wardrobe staples.
Gadget tan lines. Or if you’re like me, it’s more like sunburn lines. That’s because each summer, without fail, I somehow manage to neglect the space around my pod or my sensor, so when it’s time to remove it, there’s a huge red circle around the perimeter of where the device was situated. Maybe this year I’ll actually learn my lesson and take the time to apply sunscreen properly so I can avoid the very not-cute sunburn circles.
Travel coolers. This is probably the least obvious sign of diabetes in the summertime, but to those in the know, coolers meant to protect insulin are pretty recognizable compared to regular coolers. Whether it’s a Frio cooling pouch or another brand of insulin cooler, people with diabetes tend to carry these throughout the summer months in order to prevent insulin from spoiling due to heat exposure.
When my pod fails, it’s pretty obvious due to the fact it’ll emit a long, loud, impossible-to-miss BEEEEEEEEEEEPing sound. (Said sound tends to inspire immediate rage, but also relief because at least my device is letting me know that it’s not working properly.)
What’s less obvious is when a pod is malfunctioning, and the beeping sound doesn’t get triggered. In this context, I define “malfunctioning pod” as a pod that’s leaking insulin, or a pod that appears to have deployed the cannula correctly into my skin, but somehow it’s become dislodged.
Both of those scenarios are infuriating because they’re much more difficult to discover.
But lately, I’ve found myself dealing with both – more than likely, it’s just totally random, but it also may be due in part to the fact that I sometimes have more trouble with pods in the summertime. Heat and humidity don’t always bode well for my pod’s adhesive, and my pods have fallen victim to peeling up and off my body as a result of my sweaty summertime skin.
Since I’ve got recent experience with both types of malfunctioning pod as described above, I decided to share my tips on how to identify (and then deal with) these phenomenons:
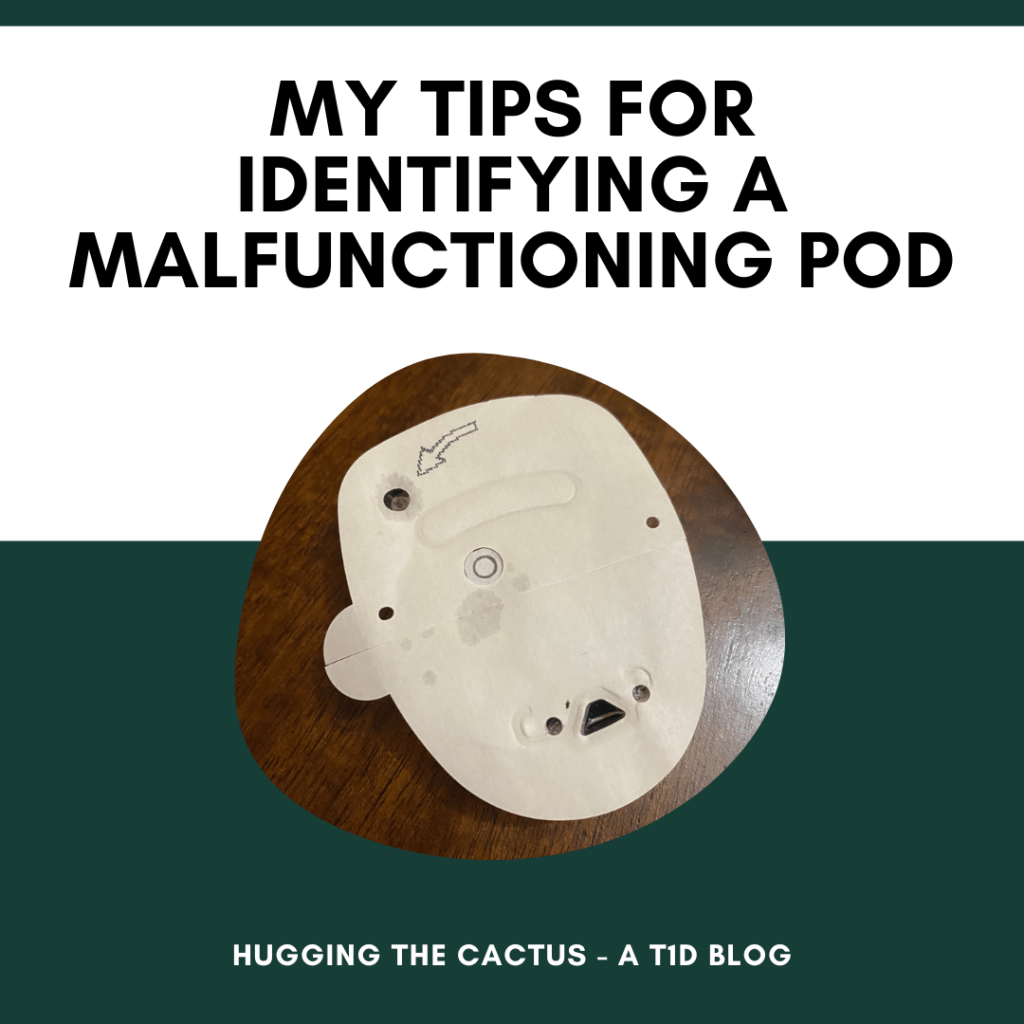
Leaky pod: The first sign that my pod is leaking insulin is my blood sugar being higher than usual. If I’m bolusing for foods that I consume on a regular basis and seeing serious spikes afterward, I check my site by lightly running my fingertips around my pod, and then sniffing them to see if I can detect the pungent scent of insulin. It might sound kind of funny to go about it that way, but it really is the best way to confirm a leak as it’s riskier to just up and rip the pod off my skin to look for puddled insulin underneath. If I do smell insulin after my sniff test, then I will go ahead and change the pod – and double confirm my suspicions by looking at the leaky pod’s adhesive at that point in time. More often than not, the adhesive will be visibly wet around where the cannula is, and that is always a signal to me that the pod was indeed leaking and therefore responsible for my high blood sugars. And on a very rare occasion, a leaky pod will be obvious before it even goes on my body (as shown in the below photo), making it much easier to handle as I can address it before it starts to negatively impact my levels.
Dislodged cannula: You would think that I would immediately know if a cannula was no longer poking my skin, but honestly, it’s difficult to tell when it gets jostled out of place! And it’s even harder to figure out if the adhesive surrounding the pod is fully intact. So what are the signs of this happening? Well, high blood sugar is the main one, but I’ve also realized that itchy skin is another. It’s strange and I don’t have an explanation for it, but when my cannula is on the cusp of ejecting (or already has), my skin gets super itchy. If I’m experiencing that itchy sensation and my adhesive has already begun to peel around the edges, I don’t even question going through with a pod change, as I’m almost always able to visually confirm that my cannula is out of place. When I don’t have that visual guidance, it’s much more of a crapshoot and I still almost always end up changing my pod in an attempt to stabilize my blood sugar levels. After removing it, I can sometimes see that the cannula was bent at a funny angle or something to that effect, but I don’t always get that verification. In that instance, I just chalk it up to a fussy pod and then do my best to move on from it.
The big takeaway here? More often than not, my pods work exactly as they should. Every now and then, though, I have to deal with one that malfunctions – whether it’s a total failure or one of the other situations I described above. I’ve found that when I’m in doubt or suspicious that my pod isn’t working right, then it’s best to troubleshoot within reason before making the judgment call to change it. I’d much rather have to change my pod prematurely in order to maintain in-range blood sugars than deal with 3 full days (the lifespan of one pod) filled with highs and frustration.
It’s said that good things come in small packages – and, at 5 foot, 3 inches, I’m inclined to agree in most cases.
But when it comes to diabetes devices, I’m not sure that saying still rings true for me.
When Tandem recently announced FDA clearance of the Tandem Mobi pump, which boasts the title of being the world’s smallest and most durable insulin delivery system, I started wondering about device sizing and best practices. As someone who tends to misplace things like my car keys and cell phone on a semi-regular basis, I usually appreciate it when my belongings are large enough to be easily visible from a distance; thereby, making them instantly locatable when I forget where I last put something down. I totally get that, as a tubed insulin pump, it’s almost impossible to misplace a Tandem Mobi (especially when it’s physically attached to a body), but I still think it’s worth thinking about the practicality of sizing for diabetes devices.
Yes, at first glance, smaller size likely means greater convenience and levels of discretion – two things that people with diabetes undoubtedly appreciate. But a pump that’s so small that it can fit inside the tiny coin pocket of my blue jeans (yes, that pocket that really serves no other purpose than to home a quarter or two) just seems like it’s begging to be lost or forgotten somewhere. Again, I’m fully acknowledging that the Mobi isn’t like my Omnipod due to the tubed versus tubeless design, but I’m imagining any component of my Omnipod system (the pod or the PDM) shrinking down in size and finding myself cringing rather than rejoicing. I just know that if either were smaller, I’d definitely be more likely to misplace my PDM more often, or fret over a teenier pod reservoir because logic dictates that a smaller pod would mean a smaller reservoir, causing a need for more frequent pod changes due to size alone.
So this begs the question: Is smaller really better when it comes to diabetes devices? Or, does small translate to convenience or annoyance for other people with diabetes? One thing’s for sure, smaller seems to be the way of the future for medical technology in general, so I may just have to get used to the idea that my diabetes devices are going to shrink over time and that I will just need to keep an open mind about that.
I graduated high school, started college at UMass Amherst, met my college friend group who I’m still close with today, and learned what it’s like to be an independent “adult” (I put that word in quotes because at the time, I thought I knew what it meant to be a responsible grownup. Boy, was I wrong).
But 2011 was also the year I hit another important milestone: It was the year that I started continuous glucose monitoring. Shout-out to my scarcely-used Facebook page for reminding me of that!
In addition to getting a kick out of how I just had to tell the word that my new device was “so sick!”, I’m glad that this reminder popped up the other day because it marks the point along my diabetes journey in which I finally decided to give technology a try. From roughly 1997-2011, I was firmly against any and all diabetes technology. I’m not sure why, other than I was terrified to try something new and surrender control to someone (let alone something) that wasn’t me or my mom. I also can’t quite remember why I decided that moment in time was right for me to try a CGM – perhaps it was motivated by my transition to college, or maybe I was just intrigued by the technology? – but I am so, so glad that I did.
I’m grateful to my 18-year-old self for making this choice because it opened the door to diabetes technology for me. Until the first time I put a CGM sensor on, I had no idea what I was missing out on in terms of access to data (meaning my blood sugar levels). I didn’t realize how powerful this information would be or how it would be a helpful little sidekick conveying information to me about my diabetes every day and night. I don’t think I can quantify the number of times this thing – and we’re talking the Dexcom G4, which had a long way to go compared to today’s G7 in terms of reliability and wear – truly saved my butt and improved my overall time in range by alerting me to highs and lows.
All that said, I don’t regret not trying technology sooner. I do believe that it was important for me to introduce myself to it when I truly felt ready. If anything, I’m proud of myself for trying a CGM, and then eventually an insulin pump, in my own time. It just means that I appreciate both of these tools and what they do for me on a daily basis that much more, because I remember all too well what life was like before them. And there was a serious difference! I can’t say that I love having two devices on my body at all times, but I can 100% attest to the fact that they’ve improved my quality of life with diabetes, hands down.
So better late than never, but today, I’m giving myself a little pat on the back for being brave 12 years ago and taking that initial first step in changing up the components in my diabetes care toolkit.
I always envied people who experienced a diabetes “honeymoon” period. I used to think, how nice it must be to have some extra time to prepare for fulltime life with diabetes and not quite rely on insulin injections right off the bat! I also always assumed that, after 25 years living with diabetes, that the honeymoon phase had absolutely skipped over me, and I was positive I’d never get to experience it.
Turns out, my diabetes – that saucy little minx – likes to keep me on my toes as it recently surprised me with an abrupt 48-hour window of time in which it seemed like my diabetes was cured.
That’s the only way I can describe what transpired. It was the strangest thing. One day, I woke up, ate breakfast, and took insulin for it – just as I always do. Except instead of my blood sugar spiking or even leveling out after eating, it started to drop, which was strange because I ate a fairly typical meal that morning. At the time, I thought nothing of it and just ate some extra carbs before my blood sugar went too low.
No big deal, right? But this phenomenon happened again, following both my lunch and dinner. It was especially inconvenient in the evening, as I had a volleyball game and wanted my number to be up so I could play. I had some fruit snacks before the game to keep my levels up, but was surprised when even after that, I was dropping by the tail end of our third and final match. I remember being out on the court, trying to track the ball as my team bumped it back and forth over the net with the other team, knowing full well that my blood sugar was going low but feeling determined to stay in the game until it was over. The moment the final whistle blew, I ran to grab even more fruit snacks, and felt both annoyed and confused by the whole situation.
The following day, I decided I wasn’t going to mess around anymore. I wanted to cut my mealtime insulin doses in half to see if that helped me at all. It was a solid idea, but it didn’t prove to do much to help as I again dropped after breakfast and lunch. Okay, so clearly that course of action wasn’t enough. Maybe I could try switching from automated mode to manual on my Omnipod 5 PDM and put myself fully in control, rather than leaving it up to technology. I set a temp basal decrease to ensure I was getting very little basal insulin, and resolved to enjoy my pizza dinner that evening with friends.
Of course, pizza is notoriously difficult to bolus for, so I knew I’d have to do even more extra work in order to prevent my blood sugar from dipping. So not only did I take half the amount of insulin than normal, but I also did an extended bolus so that I wouldn’t get it all upfront. I ate two fairly large slices of pizza and also had a generous serving of chips that I technically didn’t include in my bolus calculations. So imagine my bewilderment when, 2-3 hours post-pizza, I was still going low. I poured myself a glass of regular soda, and it became my companion for the remainder of the evening. I’d take sips as I saw my graph report blood sugars that never went higher than 110, but fluctuated for the most part between 60 and 90.
It was wild, and I was actually getting pretty worried about the whole situation. I couldn’t make sense of it. I ran through all the variables that could’ve caused this to happen – was I wearing my pod in a strange site? Was it because of my period? Could it be due to my activity levels or changes in the weather? I weighed so many possibilities in my mind and came up with nothing definitive, so I went to my next best resource for input…the diabetes online community.
I asked around for input and was – as always – so grateful to the folks who reached out and served as thought partners with me. Based on what I learned, the most likely culprit is hormonal changes. In fact, perhaps it was a bit of a birthday gift from my diabetes as I ushered in a new age/phase in life. It’s still totally bizarre that it happened, but a friend reassured me of her own experiences with the same temporary phenomenon as she’s experienced menopausal shifts. So, maybe…just maybe this was the explanation I was looking for, and perhaps the whole thing happened to signify the start of my upcoming cycle.
I won’t ever know for certain if that was indeed the cause of my temporary reprieve from diabetes, but at least I can find a little comfort in knowing that I got through it (as my blood sugars and insulin needs bounced back with a vengeance the following day) and that I had the support and feedback from friends and strangers alike the whole time.
So…remember all the times on this blog that I wrote about how important it is, as a person with diabetes, to be prepared at all times? And how it’s vital to have a back-up in case something unexpected happens with technology?
Well, apparently I don’t take my own advice. I mean, I usually do, but once in a blue moon, I am forgetful. Or negligent. In this particular scenario, I was both, because I simply didn’t pay attention to the fact that my CGM sensor was due for a change…and I was stuck at my workplace office, roughly 45 minutes from home, without my meter or a backup sensor in my bag. So when my CGM sensor expired at 1:48 in the afternoon, I realized that I wouldn’t have a means of checking my blood sugar until I returned home for the day. And I was a bit freaked out about that.
My biggest concern was that my blood sugar levels would run high and I wouldn’t know for certain or be able to do anything about it. I’d eaten more carbohydrates at lunchtime than usual, and had low confidence that I’d guessed the carb count accurately.
Instead of losing my cool or deciding to head home early, though, I impressed myself by choosing to ride it out. I felt sure that I’d be able to pick up my body’s signals if my blood sugar began to run low (which is definitely scarier than it running high for too long, anyways), and if it were high? Well, then, I’d just have to cut my losses and correct for it as soon as I got home. It’s never fun to have high blood sugar when it can be so easily fixed with an insulin dose, but given my options in this particular scenario I decided that I’d make peace with it, should that end up being my outcome.
It was a long 3ish hours, flying blind without my security blanket I mean, CGM, but I made it through and checked my blood sugar with my meter the moment I arrived home. And guess what? All that worrying about being high was for nothing because I was sitting pretty at 82 – a stellar blood sugar level in ordinary circumstances, but one that felt especially victorious after this less-than-ideal situation I got myself into.
The whole experience opened my eyes to the fact that my CGM is more than just a piece of diabetes technology to me, it’s a security blanket. It makes me feel that much more confident in making the majority of my diabetes-related decisions on a daily basis. And while it’s great that I have my CGM’s data available to me most of the time, it’s also an indication that maybe I could stand to be a little less reliant on it and trust myself and my own body a bit more. Maybe I could stand to check my graph 50% less than I do each day (believe me, I glance at it frequently, definitely more than I need to) to build a healthier boundary between me and my CGM. Or maybe I can do a better job at keeping tabs on my back-up supplies so I don’t run into this again.
Or…maybe I can totally do both of those things to do a better job of becoming my own source of security when it comes to my diabetes. I like the sound of that.
This was originally published on Hugging the Cactus on December 4, 2019. I’m sharing it again today because there have been many diabetes tech outages since then – and I’m certain there will be more in the future – but my question still remains: Do we take medical technology for granted? I ponder the answer to that below…
Alright, now that I’ve got THAT out of the way…
For the last several days, the DOC has been in a bit of a panic. And when I say “bit” I mean “a helluva lot”. That’s because the day after Thanksgiving, Dexcom Follow stopped working. This means that parents/caretakers who rely on the technology to monitor their child’s/loved one’s blood sugar levels were left in the dark. It sparked confusion, outrage, and downright fear, all of which only seemed to intensify over the weekend and into this week when the problem was only partially solved for most users.
Rather than coming together to support one another, the DOC swiftly divided into two camps: The first consisted of individuals who sought to gently remind others that this technology is still pretty new. It hasn’t even been around for two decades. That meant that for many years before then, people with diabetes were doing things the “old school” way, and getting by just fine. Doesn’t this mean that we should all be able to make it through unexpected technology blackouts, knowing that we have our blood sugar meters to fall back on?
The second camp was in a greater fury over the issue. This camp relied on the Dexcom G6 system because those within it simply didn’t know a life without the continuous glucose monitoring technology. For them, the outage was a bit like asking them to Google something without access to the Internet – it’s pretty much impossible, unless you’ve got an Encyclopedia handy. Oh, and it’s MUCH higher stakes, because people who don’t recognize symptoms of low or high blood sugar need this technology to work in order to stay on top of fluctuating blood sugar levels. Let’s not even get into how much is PAID for this expensive piece of medical equipment…one would argue that the high cost of supplies means that the technology should work at all times, no matter what.
If you’re like me, you can see that both of these groups have perfectly valid points. I’ve had diabetes long enough that I didn’t even use – and didn’t see the point in using – continuous glucose monitoring or insulin pumps until a few years ago. I took care of my diabetes the old fashioned way growing up: doing fingerstick checks multiple times per day, treating low blood sugars with 15 carbs then waiting 15 minutes, checking blood sugar levels about an hour after injecting insulin to make sure highs were coming down the way they should. This way of handling diabetes worked for me for a long, long time…throughout elementary, middle, and high school, right up to college.
Then I got a continuous glucose monitor (I believe it was the Dexcom G4) just before starting my freshman year of college. And I haven’t really been without a CGM device since then. It’s changed my life and helped me navigate adulthood with diabetes. Whenever I do experience periods of the technology not working the way it should, it’s infuriating because I feel like it’s not worth throwing away buckets of cash on it in those periods of inconsistency and inaccuracy.
But here’s what I’m wondering, as a result of this Great Dexcom G6 Outage of 2019…do we take this technology for granted?
Do we truly appreciate the times that it works the way it should?
Do we expect too much from something that, technologically speaking, still has a long way to go in terms of working perfectly?
Do we rely too heavily on continuous glucose monitors to provide us peace of mind when, in reality, they simply provide us with real-time updates of our blood sugar levels (i.e., it’s a stream of data)?
I don’t have answers to these questions. I can reflect on my own answers to them; furthermore, I can ponder how and why the DOC gets so divisive in these times where we should try to come together, listen to (and learn from) differing perspectives, and figure out what we can do to best support one another during trying times.
Those were the first words that came to mind when I learned that the Omnipod Eros system – the one that comes with a bulkier, non-touchscreen PDM – was going to be discontinued at the end of this year. (You can get more information about this decision here.)
Now, you might be wondering why I’d have that reaction, especially considering I haven’t been on the Eros system in over two years. And when I am fully aware of the fact that the Omnipod Dash and 5 systems are out, available, and the latest/greatest offerings when it comes to pump therapy from Insulet.
The main reason why I think it’s too soon to nix the Eros system? It’s because of how it affects choice. By discontinuing it, this means there’s one less option on the market for people who are interested in Omnipod’s tubeless insulin delivery. Not so much in terms of the pod itself, as that design has largely remained unchanged as Insulet innovates products over time, but certainly regarding the PDM device.
It goes without saying that the Eros PDM is clunky, uglier, and overall out-of-date compared to it’s newer counterparts. The Eros PDM is a behemoth in size that relies on AAA batteries to keep it running and features chunky buttons that need to be firmly pressed in order to navigate from one screen to the next. Meanwhile, the Dash and 5 PDMs are sleek, touchscreen models that can be charged just like a cell phone. So I can’t deny that the Eros looks like it’s from the Stone Age when comparing it to the Dash and 5.
But this is actually favorable to some people. One thing that kept me from transitioning to an insulin pump for a long time was that I didn’t want to feel super attached to yet another physical piece of equipment I’d have to carry around; at that point in my life, I was already toting around my phone and separate CGM receiver (this was pre-Dexcom app days) everywhere I went. When I finally did start using the Omnipod Eros, it took time for me to get used to the PDM, but I came to appreciate it for its distinct heft, and could quickly and easily grab it from my bag without really having to look for it due to its size.
I liked my Eros PDM so much that I have more than one image of myself holding it up in my photo archives…
Now, I constantly get my PDM and cell phone mixed up – sometimes, I even go to text someone from my PDM, only to realize after I unlock it that I grabbed the wrong device. And I hate that I have another piece of tech that needs to be recharged so frequently. I monitor the battery life all the dang time, and have to plug my PDM in every few days to fully recharge it, whereas with the Eros all I had to do was swap out the batteries every 3 or so months. It doesn’t sound like that big of a deal, but I already have so much to monitor when it comes to my diabetes that I sometimes resent that I have to also keep an eye on the technology that’s supposed to help me simplify my management.
Moreover, a reason why the Eros PDM was so bulky was that it also doubled as a blood sugar meter. Admittedly, I scarcely ever utilized it as such, but it was always nice to know that I had the option of doing so if I wanted. Since the Dash and the 5 PDMs are essentially repurposed smartphones, the blood sugar meter function isn’t available on either, and I know this is probably a bummer to some people with diabetes who preferred using the PDM device as an all-in-one type of technology.
So while I get the decision to encourage more folks to upgrade to newer Omnipod systems, I’m also a little bummed for the individuals who were deliberately postponing that move, or not wanting to make it in the first place. I can totally relate to not feeling ready to make a diabetes tech change-up; after all, I waited almost 15 years of having diabetes before I even thought about trying an insulin pump. I benefited from being able to make that transition when I felt ready, and I just feel that it’s a shame that others won’t be able to do the same due to the pending discontinuation of the Omnipod Eros.
A packed conference room. A Dexcom alert due to a low blood sugar. A girl, interrupted as she tries to reconcile what her diabetes demands and what her professional responsibilities required her to do.
A girl, interrupted by diabetes.
Oh hey, I am that girl, and I found myself in this precise scenario when I attended in-office training for my job.
It was just after noon and I was rebounding from a high blood sugar that I’d dealt with earlier in the day. We were going to break for lunch at any moment, and it wasn’t like my blood sugar was tanking – it was holding steady around 65-70 mg/dL. But it was enough to disrupt my concentration on the work presentation and throw me off-guard.
It’d been quite some time – years, honestly – since I found myself dealing with the stress of a low blood sugar in a room filled with people, most of whom I didn’t know. Likely, it hadn’t occurred since I was at my last office job. But it didn’t really matter how long ago or when, precisely, it happened – all I could think about was, how the heck did I manage lows before in workplace meetings that I couldn’t easily excuse myself from?
It might sound like I was overcomplicating matters – I could just get up and excuse myself from the room while I found a snack to treat the low – but one shortcoming that’s followed me about my diabetes and my professional journey is that I like to keep all diabetes matters as low of a priority as possible during the workday. Of course, I take care of myself by making sure I eat regularly and keeping extra supplies on-hand, but I don’t always correct my blood sugar as quickly as I might normally when I’m somewhere else, such as home. I don’t know if it’s my determination to prove to my colleagues that diabetes doesn’t interfere with my workflow or some factor that gets in my way, but I know enough that I’m able to admit that it’s a slight issue for me that I ought to work on.
So when I began to feel the shakes of an oncoming low blood sugar, that was confirmed by a buzzing Dexcom, I found myself toying between two choices: 1) Either I could excuse myself from the conference room and grab a snack, or 2) I could power through, as there was likely 20 minutes or less remaining in the session. As I deliberated, anxiety slowly crept in as I started imagining nightmare scenarios in which I passed out in front of my colleagues. That’s when *ding* the lightbulb went off over my head: I remembered the hard candies I’d pocketed earlier in the day, which I’d intended to be a bit of a post-lunch treat but then realized they’d work great as a smaller-scale low treatment just when I needed it.
I popped one in my mouth and spent the next 15 minutes doing my best to immerse myself back into the training, while also taking a moment to acknowledge that I’d made a mountain out of a molehill in this situation. I don’t need to feel so self-conscious when minor diabetes-related issues happen, whether I’m at work or anywhere else. The most important thing is that I take action in a timely manner, so I can prevent more severely disruptive scenarios from happening.